

Primary angioplasty in acute myocardial infarction with right bundle branch block: should new onset right bundle branch block be added to future guidelines as an indication for reperfusion therapy?
- PMID: 21890488
- PMCID: PMC3249219
- DOI: 10.1093/eurheartj/ehr291
Primary angioplasty in acute myocardial infarction with right bundle branch block: should new onset right bundle branch block be added to future guidelines as an indication for reperfusion therapy?
Abstract
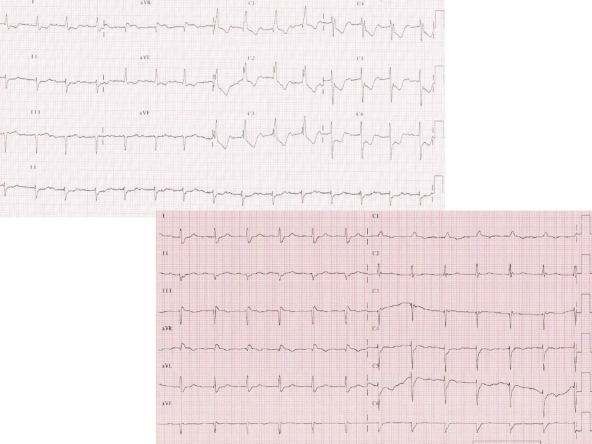
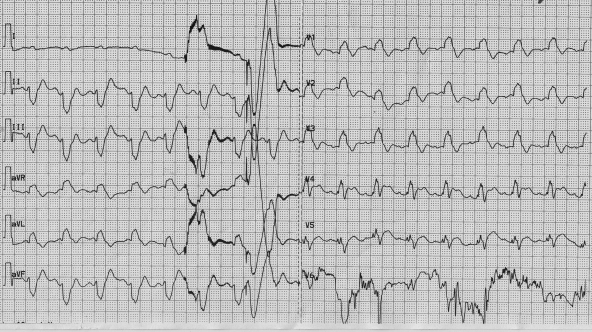
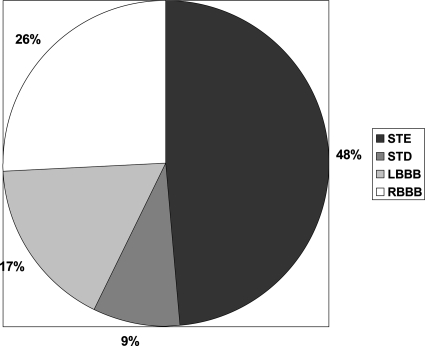
Aims: The current guidelines recommend reperfusion therapy in acute myocardial infarction (AMI) with ST-segment elevation or left bundle branch block (LBBB). Surprisingly, the right bundle branch block (RBBB) is not listed as an indication for reperfusion therapy. This study analysed patients with AMI presenting with RBBB [with or without left anterior hemiblock (LAH) or left posterior hemiblock (LPH)] and compared them with those presenting with LBBB or with other electrocardiographic (ECG) patterns. The aim was to describe angiographic patterns and primary angioplasty use in AMI patients with RBBB.
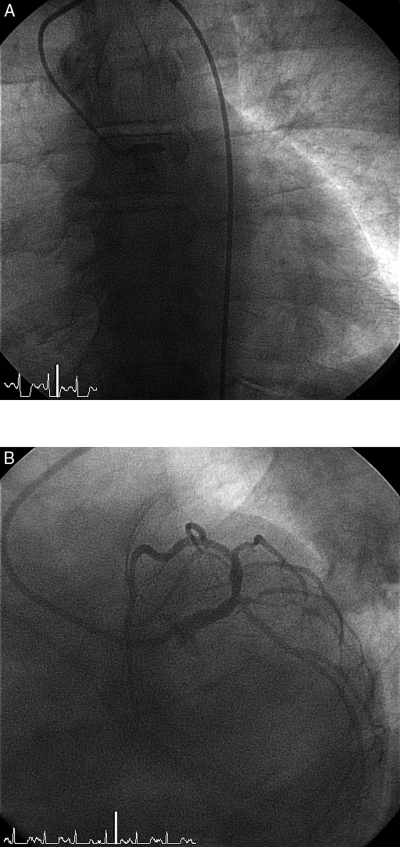
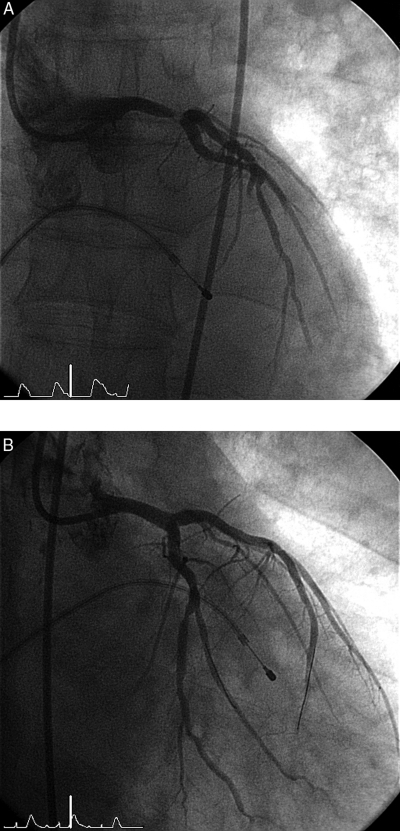
Methods and results: A cohort of 6742 patients with AMI admitted to eight participating hospitals was analysed. Baseline clinical characteristics, ECG patterns, coronary angiographic, and echocardiographic data were correlated with the reperfusion therapies used and with in-hospital outcomes. Right bundle branch block was present in 6.3% of AMI patients: 2.8% had RBBB alone, 3.2% had RBBB + LAH, and 0.3% had RBBB + LPH. TIMI flow 0 in the infarct-related artery was present in 51.7% of RBBB patients vs. 39.4% of LBBB patients (P = 0.023). Primary percutaneous coronary intervention (PCI) was performed in 80.1% of RBBB patients vs. 68.3% of LBBB patients (P< 0.001). In-hospital mortality of RBBB patients was similar to LBBB (14.3 vs. 13.1%, P = 0.661). Patients with new or presumably new blocks had the highest (LBBB 15.8% and RBBB 15.4%) incidence of cardiogenic shock from all ECG subgroups. Percutaneous coronary intervention was done more frequently (84.8%) in patients with new or presumably new RBBB when compared with other patients with blocks (old RBBB 66.0%, old LBBB 62.3%, new or presumably new LBBB 73.0%). In-hospital mortality was highest (18.8%) among patients presenting with new or presumably new RBBB, followed by new or presumably new LBBB (13.2%), old LBBB (10.1%), and old RBBB (6.4%). Among 35 patients with acute left main coronary artery occlusion, 26% presented with RBBB (mostly with LAH) on the admission ECG.
Conclusion: Acute myocardial infarction with RBBB is frequently caused by the complete occlusion of the infarct-related artery and is more frequently treated with primary PCI when compared with AMI + LBBB. In-hospital mortality of patients with AMI and RBBB is highest from all ECG presentations of AMI. Restoration of coronary flow by primary PCI may lead to resolution of the conduction delay on the discharge ECG. Right bundle branch block should strongly be considered for listing in future guidelines as a standard indication for reperfusion therapy, in the same way as LBBB.
Figures
References
-
- Wong CK, Stewart RAH, Gao W, French JK, Raffel C, White HD for the Hirulog and Early Reperfusion or Occlusion (HERO-2) Trial Investigators. Prognostic differences between different types of bundle branch block during the early phase of acute myocardial infarction: insights from the Hirulog and Early Reperfusion or Occlusion (HERO)-2 trial. Eur Heart J. 2006;27:21–28. - PubMed
-
- Van de Werf F, Bax J, Betriu A, Blomstrom-Lundqvist C, Crea F, Falk V, Filippatos G, Fox K, Huber K, Kastrati A, Rosengren A, Steg PG, Tubaro M, Verheugt F, Weidinger F, Weis M, Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K, Funck-Brentano C, Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P, Zamorano JL, Aguirre FV, Al-Attar N, Alegria E, Andreotti F, Benzer W, Breithardt O, Danchin N, Di Mario C, Dudek D, Gulba D, Halvorsen S, Kaufmann P, Kornowski R, Lip GY, Rutten F. Management of acute myocardial infarction in patients presenting with persistent ST-segment elevation: the Task Force on the Management of ST-Segment Elevation Acute Myocardial Infarction of the European Society of Cardiology. Eur Heart J. 2008;29:2909–2945. - PubMed
-
- Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC, Jr, Alpert JS, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Gregoratos G, Halperin JL, Hiratzka LF, Hunt SA, Jacobs AK. ACC/AHA Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2004;44:671–719. - PubMed
-
- Gould L, Venkataraman K, Mohhamad N, Gomprecht RF. Prognosis of right bundle-branch block in acute myocardial infarction. JAMA. 1972;219:502–503. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
