

Lack of sustained improvement in adherence or viral load following a directly observed antiretroviral therapy intervention
- PMID: 21890753
- PMCID: PMC3189166
- DOI: 10.1093/cid/cir537
Lack of sustained improvement in adherence or viral load following a directly observed antiretroviral therapy intervention
Abstract
Background: Methadone clinic-based directly observed antiretroviral therapy (DOT) has been shown to be more efficacious for improving adherence and suppressing human immunodeficiency virus (HIV) load than antiretroviral self-administration. We sought to determine whether the beneficial effects of DOT remain after DOT is discontinued.
Methods: We conducted a post-trial cohort study of 65 HIV-infected opioid-dependent adults who had completed a 24-week randomized controlled trial of methadone clinic-based DOT versus treatment as usual (TAU). For 12 months after DOT discontinuation, we assessed antiretroviral adherence using monthly pill counts and electronic monitors. We also assessed viral load at 3, 6, and 12 months after DOT ended. We examined differences between DOT and TAU in (1) adherence, (2) viral load, and (3) proportion of participants with viral load of <75 copies/mL.
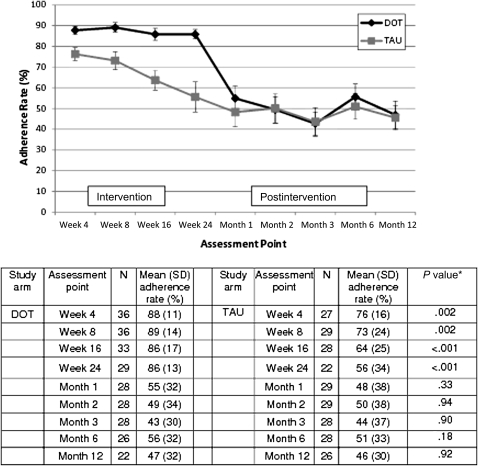
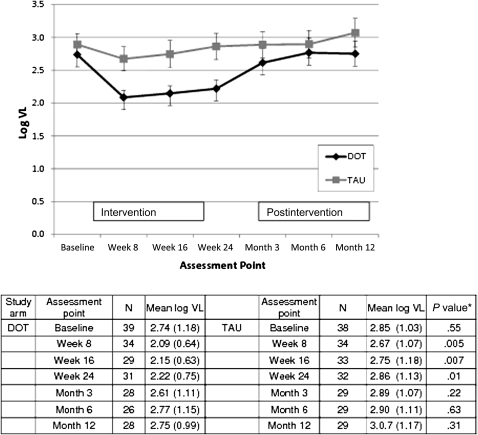
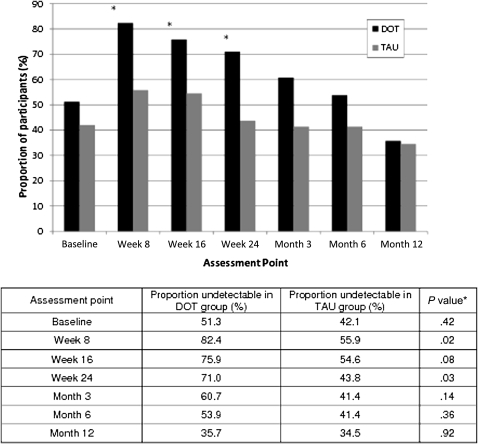
Results: At trial end, adherence was higher among DOT participants than among TAU participants (86% and 54%, respectively; P < .001), and more DOT participants than TAU participants had viral loads of <75 copies/mL (71% and 44%, respectively; P = .03). However, after DOT ended, differences in adherence diminished by 1 month (55% for DOT vs 48% for TAU; P = .33) and extinguished completely by 3 months (49% for DOT vs 50% for TAU; P = .94). Differences in viral load between DOT and TAU disappeared by 3 months after the intervention, and the proportion of DOT participants with undetectable viral load decreased steadily after DOT was stopped until there was no difference (36% for DOT and 34% for TAU; P = .92).
Conclusions: Because the benefits of DOT for adherence and viral load among HIV-infected methadone patients cease after DOT is stopped, methadone-based DOT should be considered a long-term intervention.
Figures
References
-
- Behforouz HL, Kalmus A, Scherz CS, Kahn JS, Kadakia MB, Farmer PE. Directly observed therapy for HIV antiretroviral therapy in an urban US setting. J Acquir Immune Defic Syndr. 2004;36:642–5. - PubMed
-
- Altice FL, Mezger JA, Hodges J, et al. Developing a directly administered antiretroviral therapy intervention for HIV-infected drug users: implications for program replication. Clin Infect Dis. 2004;38:S376–87. - PubMed
-
- Mitty JA, Macalino GE, Bazerman LB, et al. The use of community-based modified directly observed therapy for the treatment of HIV-infected persons. J Acquir Immune Defic Syndr. 2005;39:545–50. - PubMed
-
- Khanlou H, Kandula VR, Yeh V, et al. Pilot study of directly observed therapy in highly nonadherent HIV-infected patients in an urban community-based institution. J Acquir Immune Defic Syndr. 2003;33:651–3. - PubMed
-
- Ma M, Brown BR, Coleman M, Kibler JL, Loewenthal H, Mitty JA. The feasibility of modified directly observed therapy for HIV-seropositive African American substance users. AIDS Patient Care STDS. 2008;22:139–46. - PubMed
