

Successful downstaging of high rectal and recto-sigmoid cancer by neo-adjuvant chemo-radiotherapy
- PMID: 21892276
- PMCID: PMC3161699
- DOI: 10.4137/cmo.s348
Successful downstaging of high rectal and recto-sigmoid cancer by neo-adjuvant chemo-radiotherapy
Abstract
Purpose: The benefit of neoadjuvant therapy for tumours above the peritoneal reflection is not clear. The purpose of this study is to demonstrate the feasibility and downstaging of treating locally advanced tumours from high rectum to distal sigmoid with preoperative chemoradiotherapy (CRT).
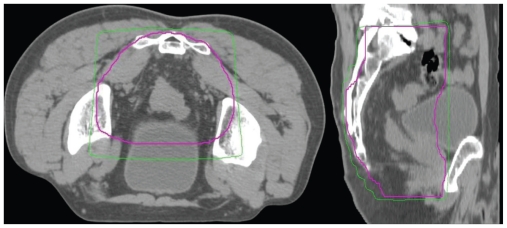
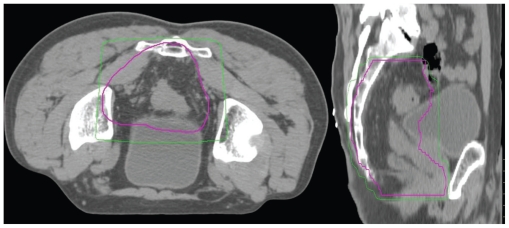
Methods and materials: Seventeen patients with high rectal, rectosigmoid or distal sigmoid tumours above the peritoneal reflection received neoadjuvant CRT, selected on MRI findings indicating T4 disease or threatened circumferential resection margin. All patients were administered neoadjuvant chemotherapy, with Oxaliplatin or Mitomycin C and a Fluoropyrimidine. The pelvis received long-course CT-planned conformal RT, 45 Gy in 25 fractions, with a boost of 5.4-9 Gy in 3-5 fractions. Thirteen patients were treated with concomitant oral or intravenous Fluoropyrimidine chemotherapy.
Results: Median follow-up was 37 months. Overall survival was 82.35% (95% Confidence Interval (CI) 54.7-93.9) and disease free survival 81.25% (95% CI 52.5-93.5). Only 1 patient suffered loco-regional relapse. Chemotherapy regimens were well tolerated, though some patients required dose reductions. Nine patients (52.9%) lowered pathologic disease AJCC stage, i.e. 'downstaged'. Six patients (35.3%) achieved complete pathological response. Clear margins were attained in all but 1 patient. Three patients were converted from cT4 to ypT3. No patient required a gap during CRT. One patient suffered a grade III acute toxicity, but no grade IV (RTOG). There were 3 grade III and 3 grade IV late toxicities (LENT-SOMA).
Conclusions: Locally advanced high rectal and recto-sigmoid tumours may be treated with pre-operative CRT with acceptable toxicity, impressive down-staging, and clear surgical margins.
Keywords: chemoradiotherapy; chemotherapy; downstaging; radiotherapy; total mesorectal excision.
Figures




References
-
- ICRU report 50: Prescribing, recording and reporting photon beam therapy. ICRU; Bethesda, MD: 1993.
-
- Improved survival with preoperative radiotherapy in resectable rectal cancer. Swedish Rectal Cancer Trial. N Engl J Med. 1997;336:980–7. - PubMed
-
- Adjuvant radiotherapy for rectal cancer: a systematic overview of 8,507 patients from 22 randomised trials. Lancet. 2001;358:1291–304. - PubMed
-
- AJCC Cancer Staging Handbook. Sixth edition. American Joint Committe on Cancer; 2002.
-
- Balch GC, Mithani SK, Shyr Y, et al. Prognostic significance of response to neoadjuvant chemoradiation therapy for rectal cancer. ASCO Annual Meeting, abstr. 2003;1047
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
