

Maintaining optimal oxygen saturation in premature infants
- PMID: 21892344
- PMCID: PMC3138176
- DOI: 10.7812/TPP/11.998
Maintaining optimal oxygen saturation in premature infants
Abstract
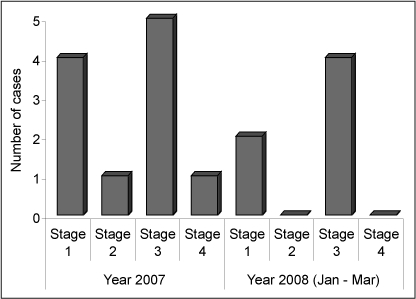
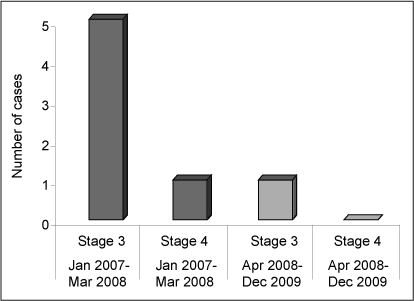
Introduction: Advances in technology have resulted in increasing survival rates for premature infants. Oxygen therapy is commonly used in neonatal units as part of respiratory support. The number of premature infants in our institution surviving with severe (stage ≥3) retinopathy of prematurity (ROP) prompted a review of oxygen therapy as a contributing factor. Prolonged exposure to high concentrations of oxygen may cause irreversible damage to the eyes of very-low-birth-weight preterm infants and is a potential cause of blindness.
Objective: We developed strategies to reduce incidence of severe ROP requiring laser surgery in premature infants.
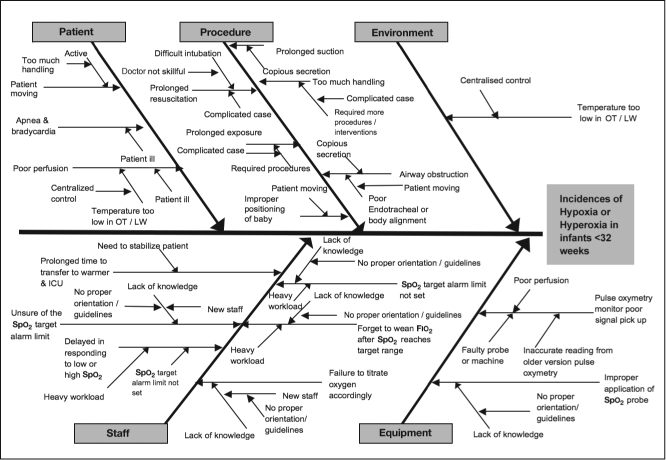
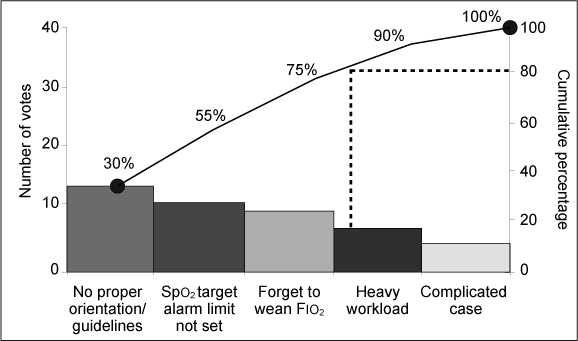
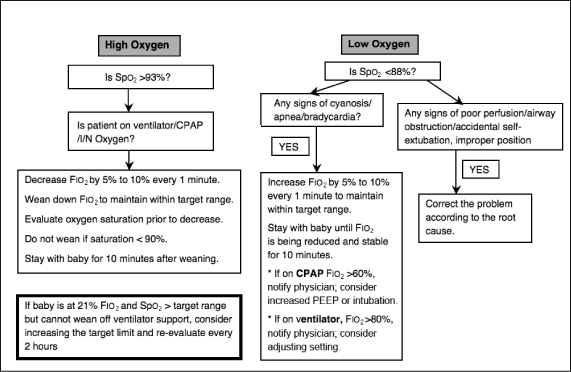
Methods: We studied 37 preterm infants who were born at a gestational age of <32 weeks, with a birth weight of <1500 g, receiving supplemental oxygen, and had been admitted to our neonatal intensive care unit. Infants received oxygen via mechanical ventilator, nasal continuous positive airway pressure (CPAP), or intranasal (I/N) and titration of oxygen was based on each infant's measured oxygen saturation (Spo(2)). For each infant, we monitored the Spo(2) trend, Spo(2) alarm limit, and the percentage of time that the alarm limit was set incorrectly. We implemented a Spo(2) targeting protocol and developed an algorithm for titrating fraction of inspired oxygen (Fio(2)).
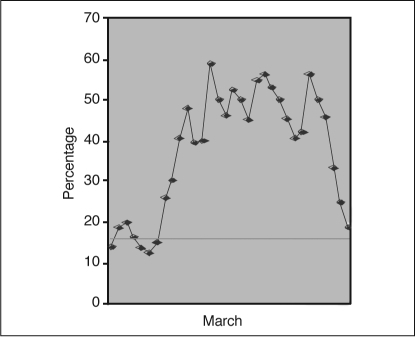
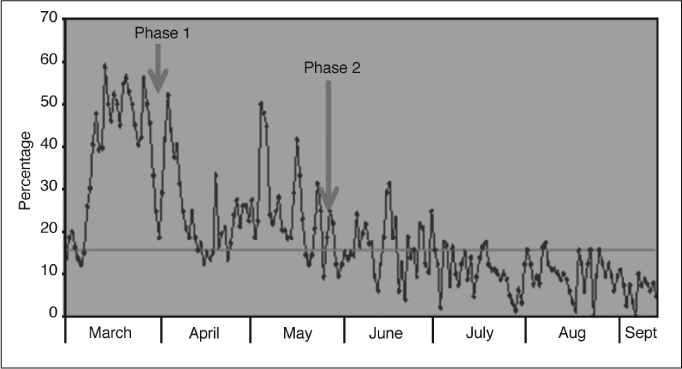
Results: After phase 1 of implementation, the percentage of time that Spo(2) readings were >95% was reduced to between 20% and 50%. However, our findings raised concern regarding the wide fluctuation of Spo(2) readings because of inconsistency in Fio(2) titration, which can contribute to deviation from the optimal target range. Accordingly, we developed an algorithm for titrating Fio(2) aimed at maintaining each infant's Spo(2) within the optimal target range. After phase 2 of implementation, the percentage of Spo(2) readings >95% was markedly reduced to between 0% and 15%. The incidence of infants with severe ROP requiring laser surgery decreased from 5 to 1.
Conclusions: A change in clinical practice aimed at maintaining oxygen within the target range to avoid a high Spo(2) was associated with a significant decrease in the incidence of both severe ROP and the need for laser surgery, thus reducing hospital costs and length of hospital stays for premature infants.
Figures

References
-
- Pollan C. Retinopathy of prematurity: an eye toward better outcomes. Neonatal Netw. 2009 Mar–Apr;28(2):93–101. - PubMed
-
- Saugstad OD. Is oxygen more toxic than currently believed? Pediatrics. 2001 Nov;108(5):1203–5. - PubMed
-
- Coe K, Butler M, Reavis N, et al. Special Premie Oxygen Targeting (SPOT): a program to decrease the incidence of blindness in infants with retinopathy of prematurity. J Nurs Care Qual. 2006 Jul–Sep;21(3):230–5. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
