

doi: 10.1016/j.ccep.2010.10.012.
Overview of Basic Mechanisms of Cardiac Arrhythmia
Affiliations
- PMID: 21892379
- PMCID: PMC3164530
- DOI: 10.1016/j.ccep.2010.10.012
Item in Clipboard
Overview of Basic Mechanisms of Cardiac Arrhythmia
Card Electrophysiol Clin.
.
No abstract available
Conflict of interest statement
Conflict of interest: None.
Figures
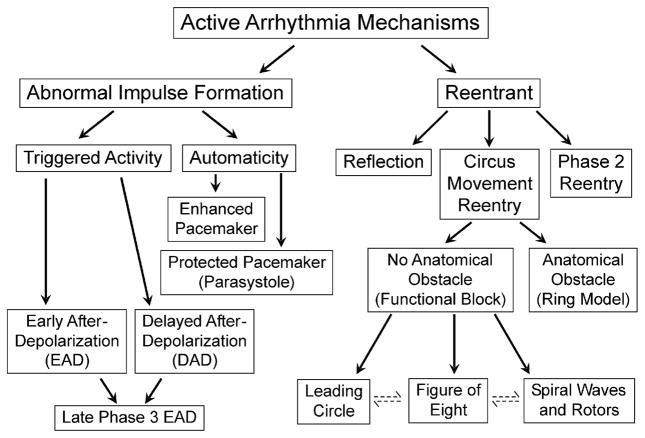
Classification of active cardiac arrhythmias.
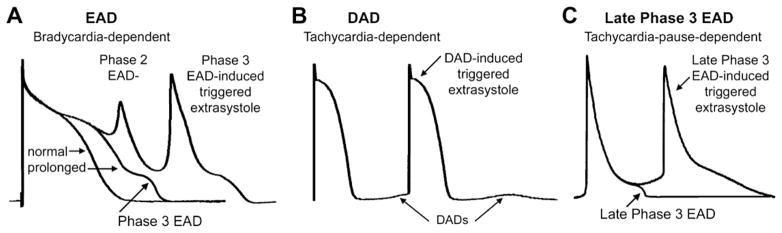
Examples of early afterdepolarization (EAD) (A), delayed afterdepolarization (DAD) (B), and late phase 3 EAD (C). (Modified from Burashnikov A, Antzelevitch C. Late-phase 3 EAD. A unique mechanism contributing to initiation of atrial fibrillation. Pacing Clin Electrophysiol 2006;29:290–5; with permission.)
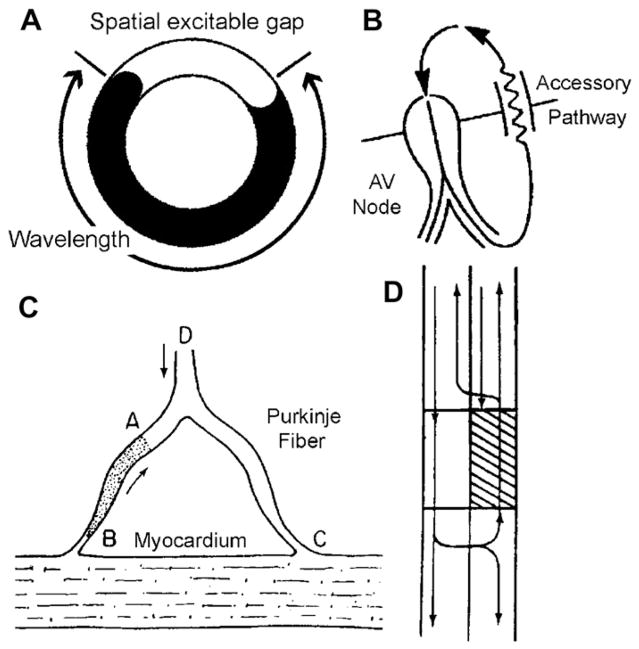
Ring models of reentry. (A) Schematic of a ring model of reentry. (B) Mechanism of reentry in the Wolf-Parkinson-White syndrome involving the AV node and an atrioventricular accessory pathway (AP). (C) A mechanism for reentry in a Purkinje-muscle loop proposed by Schmitt and Erlanger. The diagram shows a Purkinje bundle (D) that divides into 2 branches, both connected distally to ventricular muscle. Circus movement was considered possible if the stippled segment, A → B, showed unidirectional block. An impulse advancing from D would be blocked at A, but would reach and stimulate the ventricular muscle at C by way of the other terminal branch. The wavefront would then reenter the Purkinje system at B traversing the depressed region slowly so as to arrive at A following expiration of refractoriness. (D) Schematic representation of circus movement reentry in a linear bundle of tissue as proposed by Schmitt and Erlanger. The upper pathway contains a depressed zone (shaded) that serves as a site of unidirectional block and slow conduction. Anterograde conduction of the impulse is blocked in the upper pathway but succeeds along the lower pathway. Once beyond the zone of depression, the impulse crosses over through lateral connections and reenters through the upper pathway. (C and D from Schmitt FO, Erlanger J. Directional differences in the conduction of the impulse through heart muscle and their possible relation to extrasystolic and fibrillary contractions. Am J Physiol 1928;87:326–47.)
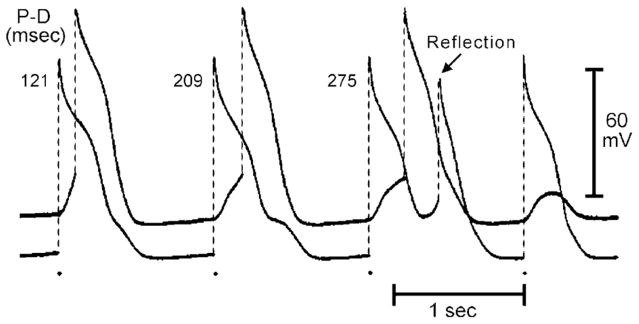
Delayed transmission and reflection across an inexcitable gap created by superfusion of the central segment of a Purkinje fiber with an ion-free isotonic sucrose solution. The 2 traces were recorded from proximal (P) and distal (D) active segments. P–D conduction time (indicated in the upper portion of the figure, in ms) increased progressively with a 4:3 Wenckebach periodicity. The third stimulated proximal response was followed by a reflection. (From Antzelevitch C. Clinical applications of new concepts of parasystole, reflection, and tachycardia. Cardiol Clin 1983;1:39–50; with permission.)
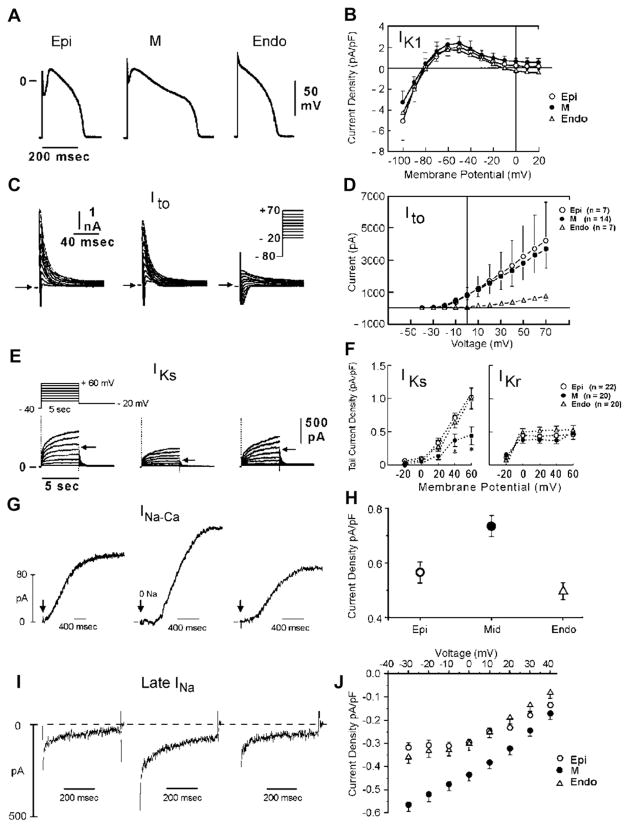
(A) Ionic distinctions among epicardial, M, and endocardial cells. Action potentials recorded from myocytes isolated from the epicardial, endocardial, and M regions of the canine left ventricle. (B) I-V relations for IK1 in epicardial, endocardial, and M region myocytes. Values are mean ± SD. (C) Transient outward current (Ito) recorded from the 3 cell types (current traces recorded during depolarizing steps from a holding potential of −80 mV to test potentials ranging between −20 and +70 mV). (D) The average peak current-voltage relationship for Ito for each of the 3 cell types. Values are mean ± SD. (E) Voltage-dependent activation of the slowly activating component of the delayed rectifier K+ current (IKs) (currents were elicited by the voltage pulse protocol shown in the inset; Na+-, K+-, and Ca2+- free solution). (F) Voltage dependence of IKs (current remaining after exposure to E-4031) and IKr (E-4031-sensitive current). Values are mean ± SE. *P < .05 compared with Epi or Endo. (G) Reverse-mode sodium-calcium exchange currents recorded in potassium- and chloride-free solutions at a voltage of −80 mV. INa-Ca was maximally activated by switching to sodium-free external solution at the time indicated by the arrow. (H) Midmyocardial sodium-calcium exchanger density is 30% greater than endocardial density, calculated as the peak outward INa-Ca normalized by cell capacitance. Endocardial and epicardial densities were not significantly different. (I) TTX-sensitive late sodium current. Cells were held at −80 mV and briefly pulsed to −45 mV to inactivate fast sodium current before stepping to −10 mV. (J) Normalized late sodium current measured 300 msec into the test pulse was plotted as a function of test pulse potential. (Data from Zygmunt AC, Goodrow RJ, Antzelevitch C. INaCa contributes to electrical heterogeneity within the canine ventricle. Am J Physiol Heart Circ Physiol 2000;278:H1671;8; and Refs.,,)
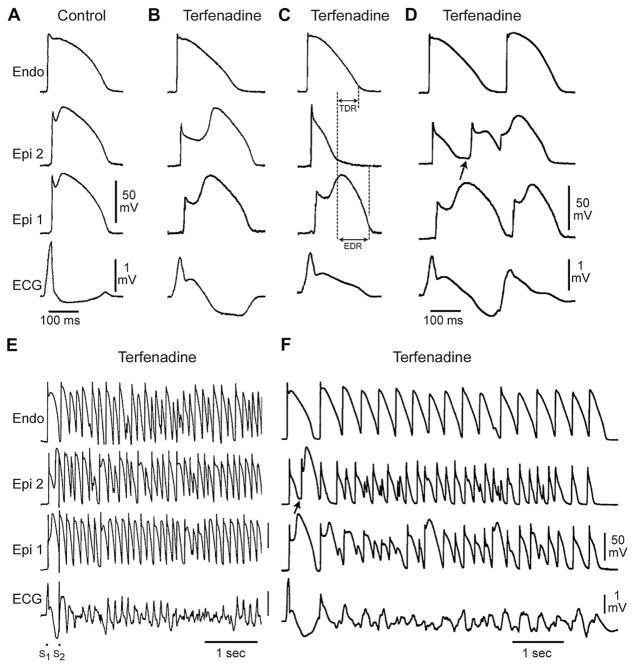
Cellular basis for electrocardiographic and arrhythmic manifestation of BrS. Each panel shows transmembrane action potentials from 1 endocardial (top) and 2 epicardial sites together with a transmural ECG recorded from a canine coronary-perfused right ventricular wedge preparation. (A) Control (basic cycle length (BCL) 400 msec). (B) Combined sodium and calcium channel block with terfenadine (5 μM) accentuates the epicardial action potential notch creating a transmural voltage gradient that manifests as an ST segment elevation or exaggerated J wave in the ECG. (C) Continued exposure to terfenadine results in all-or-none repolarization at the end of phase 1 at some epicardial sites but not others, creating a local epicardial dispersion of repolarization (EDR) as well as a transmural dispersion of repolarization (TDR). (D) Phase 2 reentry occurs when the epicardial action potential dome propagates from a site where it is maintained to regions where it has been lost giving rise to a closely coupled extrasystole. (E) Extrastimulus (S1–S2 = 250 msec) applied to epicardium triggers a polymorphic VT. (F) Phase 2 reentrant extrasystole triggers a brief episode of polymorphic VT. (Modified from Fish JM, Antzele-vitch C. Role of sodium and calcium channel block in unmasking the Brugada syndrome. Heart Rhythm 2004;1:210–17; with permission.)
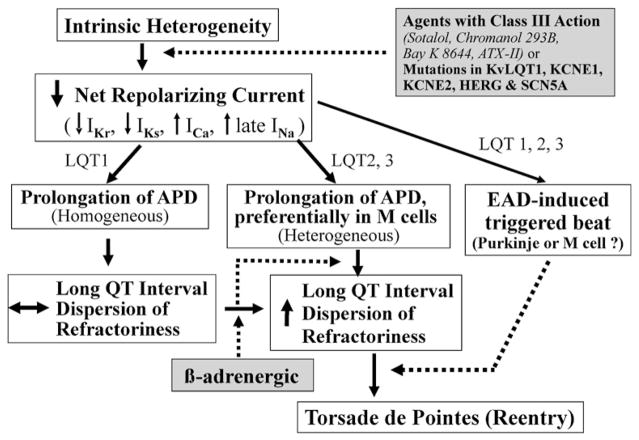
Proposed cellular and ionic mechanisms for the long QT syndrome.
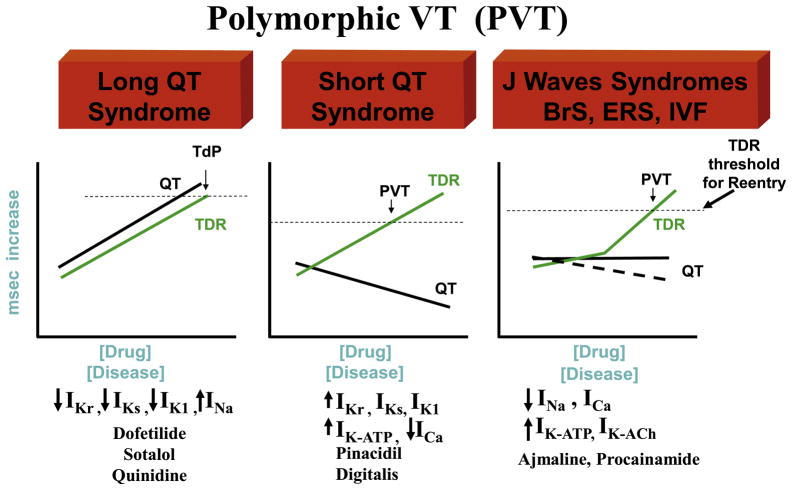
The role of transmural dispersion of repolarization (TDR) in channelopathy-induced sudden death. In the long QT syndrome, QT increases as a function of disease or drug concentration. In the J wave syndromes (Brugada and early repolarization syndromes), it remains largely unchanged or is moderately abbreviated, and in the short QT syndrome, QT interval decreases as a function of disease or drug. The 3 syndromes have in common the ability to amplify TDR, which results in the development of polymorphic VT (PVT) or Torsade de Pontes (TdP) when dispersion reaches the threshold for reentry.
References
-
- Maltsev VA, Vinogradova TM, Lakatta EG. The emergence of a general theory of the initiation and strength of the heartbeat. J Pharmacol Sci. 2006;100:338–69. - PubMed
-
- DiFrancesco D. The pacemaker current If plays an important role in regulating SA node pacemaker activity. Cardiovasc Res. 1995;30:307–8. - PubMed
-
- Levy MN. Sympathetic-parasympathetic interactions in the heart. Circ Res. 1971;29:437–45. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
