

Impact of mammographic screening on the detection of good and poor prognosis breast cancers
- PMID: 21892702
- PMCID: PMC5646368
- DOI: 10.1007/s10549-011-1748-z
Impact of mammographic screening on the detection of good and poor prognosis breast cancers
Abstract
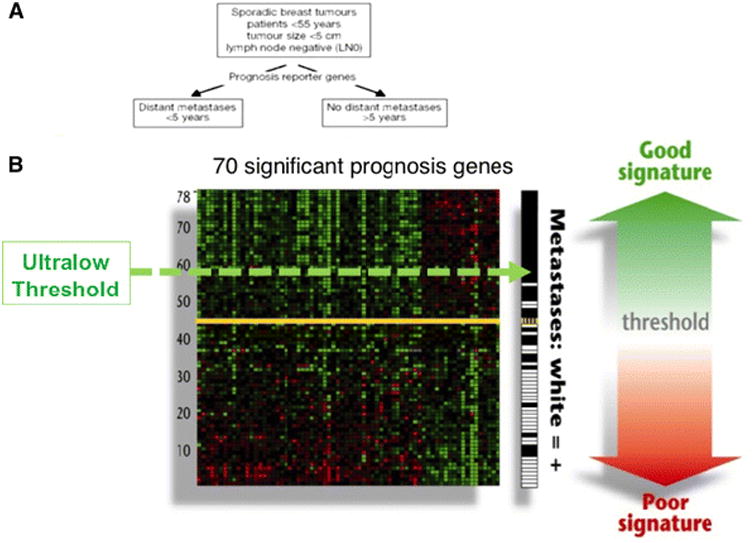
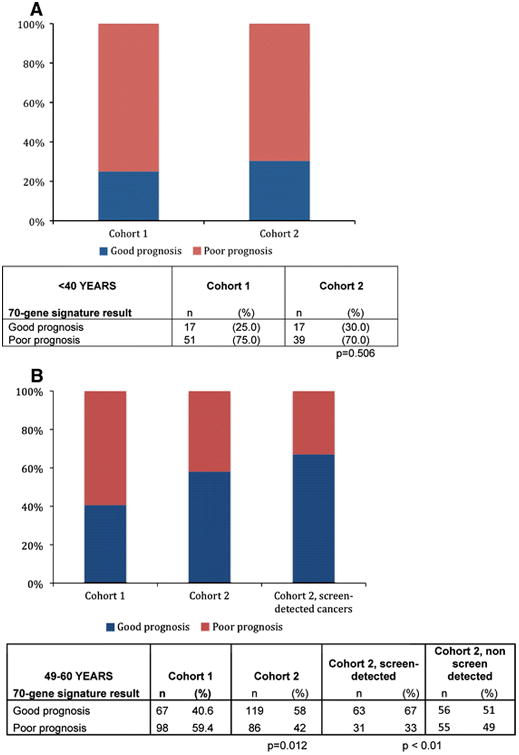
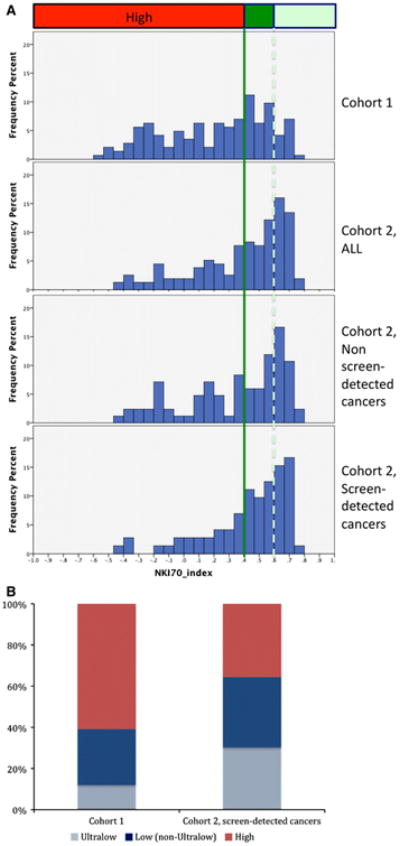
We sought to compare the molecular signature of node negative cancers from two cohorts 15 years apart, to determine if there is molecular evidence of increase in low and ultralow risk cancers over time. We studied the impact of age, time period of diagnosis, and mammographic screening on biology of tumors where The Netherlands Cancer Institute 70-gene prognosis signature was generated as part of 2 validation series, one retrospective (1984-1992), Cohort 1, and one prospective (2004-2006), Cohort 2. A total of 866 patients were analyzed. Regardless of time period of diagnosis, the proportion of T1, grade 1, hormone receptor positive (HR) tumors, and good prognosis by 70-gene signature significantly increases as age increases (P < 0.01). In women aged 49-60, the time period of diagnosis significantly affects the proportion of cancers that were NKI 70-gene low risk: 40.6% (67/165) compared with 58% (119/205) for Cohorts 1 and 2, respectively. This is in contrast to the absence of a significant change for women under age 40, where 25% (17/68) and 30% (17/56) were low risk in Cohorts 1 and 2, respectively. In women aged 49-60, using an ultralow risk threshold of the 70-gene signature, 10% of tumors in Cohort 1 were ultralow risk compared with 30% for women with screen-detected cancers in Cohort 2. Older age and method of detection (screening) are associated with a higher likelihood of a biologically low risk tumor. In women over age 50, biologically low risk tumors are frequent and tools that classify risk may minimize overtreatment.
Figures
References
-
- Esserman L, Shieh Y, Thompson I. Rethinking screening for breast cancer and prostate cancer. JAMA. 2009;302(15):1685–1692. - PubMed
-
- Welch HG, Black WC. Overdiagnosis in cancer. J Natl Cancer Inst. 2010;102(9):605–613. - PubMed
-
- Ravdin PM, et al. Computer program to assist in making decisions about adjuvant therapy for women with early breast cancer. J Clin Oncol. 2001;19(4):980–991. - PubMed
-
- Paik S, et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med. 2004;351(27):2817–2826. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
