

Comparative efficacy and safety of 4 randomized regimens to treat early Pseudomonas aeruginosa infection in children with cystic fibrosis
- PMID: 21893650
- PMCID: PMC3991697
- DOI: 10.1001/archpediatrics.2011.136
Comparative efficacy and safety of 4 randomized regimens to treat early Pseudomonas aeruginosa infection in children with cystic fibrosis
Abstract
Objective: To investigate the efficacy and safety of 4 antipseudomonal treatments in children with cystic fibrosis with recently acquired Pseudomonas aeruginosa infection.
Design: Randomized controlled trial.
Setting: Multicenter trial in the United States.
Participants: Three hundred four children with cystic fibrosis aged 1 to 12 years within 6 months of P aeruginosa detection.
Interventions: Participants were randomized to 1 of 4 antibiotic regimens for 18 months (six 12-week quarters) between December 2004 and June 2009. Participants randomized to cycled therapy received tobramycin inhalation solution (300 mg twice a day) for 28 days, with oral ciprofloxacin (15-20 mg/kg twice a day) or oral placebo for 14 days every quarter, while participants randomized to culture-based therapy received the same treatments only during quarters with positive P aeruginosa cultures.
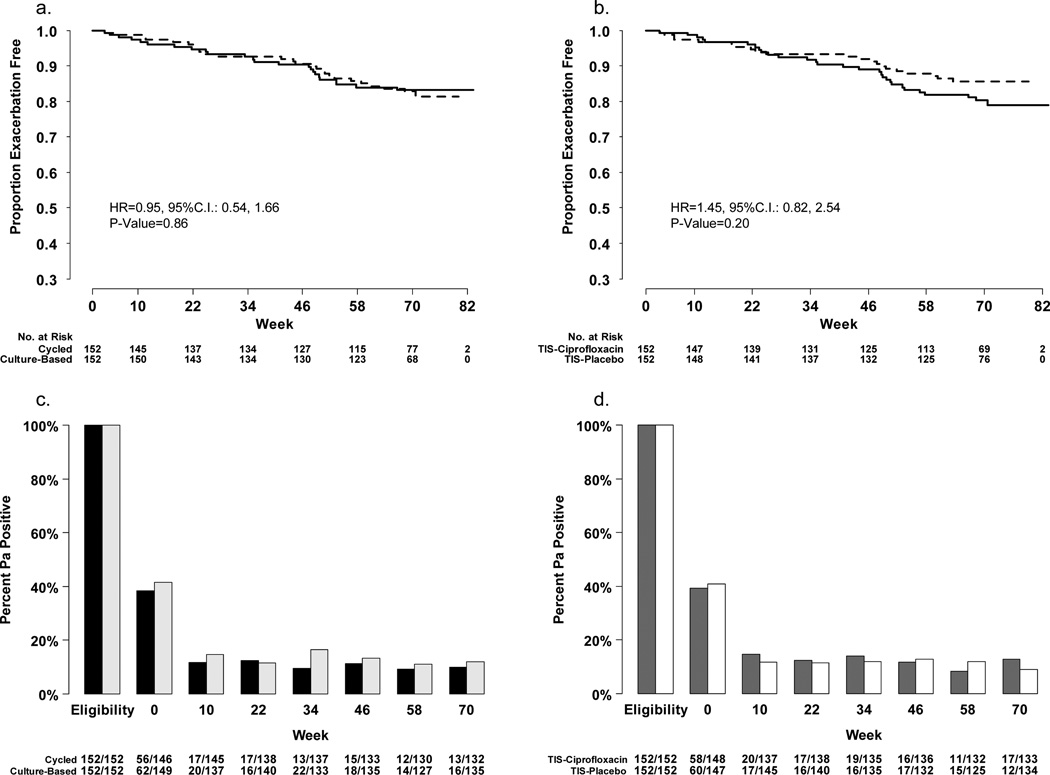
Main outcome measures: The primary end points were time to pulmonary exacerbation requiring intravenous antibiotics and proportion of P aeruginosa -positive cultures.
Results: The intention-to-treat analysis included 304 participants. There was no interaction between treatments. There were no statistically significant differences in exacerbation rates between cycled and culture-based groups (hazard ratio, 0.95; 95% confidence interval [CI], 0.54-1.66) or ciprofloxacin and placebo (hazard ratio, 1.45; 95% CI, 0.82-2.54). The odds ratios of P aeruginosa- positive culture comparing the cycled vs culture-based group were 0.78 (95% CI, 0.49-1.23) and 1.10 (95% CI, 0.71-1.71) comparing ciprofloxacin vs placebo. Adverse events were similar across groups.
Conclusions: No difference in the rate of exacerbation or prevalence of P aeruginosa positivity was detected between cycled and culture-based therapies. Adding ciprofloxacin produced no benefits.
Trial registration: ClinicalTrials.gov Identifier: NCT00097773.
Figures


Comment in
-
What have we learned about early treatment of Pseudomonas aeruginosa infection in infants and children with cystic fibrosis?Arch Pediatr Adolesc Med. 2011 Sep;165(9):867-8. doi: 10.1001/archpediatrics.2011.133. Arch Pediatr Adolesc Med. 2011. PMID: 21893653 No abstract available.
References
-
- Doring G, Conway SP, Heijerman HG, et al. Antibiotic therapy against Pseudomonas aeruginosa in cystic fibrosis: a European consensus. Eur Respir J. 2000 Oct;16(4):749–767. - PubMed
-
- Henry RL, Mellis CM, Petrovic L. Mucoid Pseudomonas aeruginosa is a marker of poor survival in cystic fibrosis. Pediatr Pulmonol. 1992 Mar;12(3):158–161. - PubMed
-
- Emerson J, Rosenfeld M, McNamara S, Ramsey B, Gibson RL. Pseudomonas aeruginosa and other predictors of mortality and morbidity in young children with cystic fibrosis. Pediatr Pulmonol. 2002;34(2):91–100. - PubMed
-
- Rosenfeld M, Gibson RL, McNamara S, et al. Early pulmonary infection, inflammation, and clinical outcomes in infants with cystic fibrosis. Pediatr Pulmonol. 2001;32(5):356–366. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- 1UL1-RR025744/RR/NCRR NIH HHS/United States
- M01-RR02172/RR/NCRR NIH HHS/United States
- UL1 RR025780/RR/NCRR NIH HHS/United States
- 1UL1-RR025780/RR/NCRR NIH HHS/United States
- M01 RR002172/RR/NCRR NIH HHS/United States
- UL1 RR025011/RR/NCRR NIH HHS/United States
- UL1 RR025014/RR/NCRR NIH HHS/United States
- U01-HL080310/HL/NHLBI NIH HHS/United States
- U01 HL080310/HL/NHLBI NIH HHS/United States
- UL1 RR024979/RR/NCRR NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- UL1-RR025011/RR/NCRR NIH HHS/United States
- ULI-RR025014-03/RR/NCRR NIH HHS/United States
- UL1-RR0024979/RR/NCRR NIH HHS/United States
- UL1 RR025744/RR/NCRR NIH HHS/United States
- UL1-RR025005/RR/NCRR NIH HHS/United States
- UL1RR025747/RR/NCRR NIH HHS/United States
- UL1 RR025747/RR/NCRR NIH HHS/United States
- UL1 RR024975/RR/NCRR NIH HHS/United States
- 1UL-RR024975/RR/NCRR NIH HHS/United States
