

Phase II and pharmacogenomics study of enzastaurin plus temozolomide during and following radiation therapy in patients with newly diagnosed glioblastoma multiforme and gliosarcoma
- PMID: 21896554
- PMCID: PMC3223090
- DOI: 10.1093/neuonc/nor130
Phase II and pharmacogenomics study of enzastaurin plus temozolomide during and following radiation therapy in patients with newly diagnosed glioblastoma multiforme and gliosarcoma
Abstract
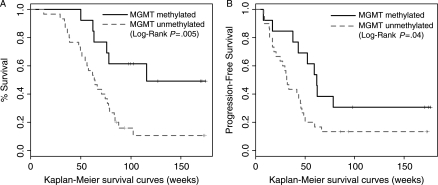
This open-label, single-arm, phase II study combined enzastaurin with temozolomide plus radiation therapy (RT) to treat glioblastoma multiforme (GBM) and gliosarcoma. Adults with newly diagnosed disease and Karnofsky performance status (KPS) ≥ 60 were enrolled. Treatment was started within 5 weeks after surgical diagnosis. RT consisted of 60 Gy over 6 weeks. Temozolomide was given at 75 mg/m(2) daily during RT and then adjuvantly at 200 mg/m(2) daily for 5 days, followed by a 23-day break. Enzastaurin was given once daily during RT and in the adjuvant period at 250 mg/day. Cycles were 28 days. The primary end point was overall survival (OS). Progression-free survival (PFS), toxicity, and correlations between efficacy and molecular markers analyzed from tumor tissue samples were also evaluated. A prospectively planned analysis compared OS and PFS of the current trial with outcomes from 3 historical phase II trials that combined novel agents with temozolomide plus RT in patients with GBM or gliosarcoma. Sixty-six patients were enrolled. The treatment regimen was well tolerated. OS (median, 74 weeks) and PFS (median, 36 weeks) results from the current trial were comparable to those from a prior phase II study using erlotinib and were significantly better than those from 2 other previous studies that used thalidomide or cis-retinoic acid, all in combination with temozolomide plus RT. A positive correlation between O-6-methylguanine-DNA methyltransferase promoter methylation and OS was observed. Adjusting for age and KPS, no other biomarker was associated with survival outcome. Correlation of relevant biomarkers with OS may be useful in future trials.
Figures

References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–996. doi:10.1056/NEJMoa043330. - DOI - PubMed
-
- Collins I, Workman P. New approaches to molecular cancer therapeutics. Nat Chem Biol. 2006;2:689–700. doi:10.1038/nchembio840. - DOI - PubMed
-
- Stupp R, Hegi ME, Gilbert MR, Chakravarti A. Chemoradiotherapy in malignant glioma: standard of care and future directions. J Clin Oncol. 2007;25:4127–4136. doi:10.1200/JCO.2007.11.8554. - DOI - PubMed
-
- Teicher BA, Alvarez E, Mendelsohn LG, Ara G, Menon K, Ways DK. Enzymatic rationale and preclinical support for a potent protein kinase C beta inhibitor in cancer therapy. Adv Enzyme Regul. 1999;39:313–327. doi:10.1016/S0065-2571(98)00026-0. - DOI - PubMed
-
- Jarvis WD, Grant S. Protein kinase C targeting in antineoplastic treatment strategies. Invest New Drugs. 1999;17:227–240. doi:10.1023/A:1006328303451. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
