

A randomized trial of the efficacy and safety of sequential intravenous/oral moxifloxacin monotherapy versus intravenous piperacillin/tazobactam followed by oral amoxicillin/clavulanate for complicated skin and skin structure infections
- PMID: 21896561
- PMCID: PMC3191944
- DOI: 10.1093/jac/dkr344
A randomized trial of the efficacy and safety of sequential intravenous/oral moxifloxacin monotherapy versus intravenous piperacillin/tazobactam followed by oral amoxicillin/clavulanate for complicated skin and skin structure infections
Abstract
Objectives: The primary aim of the RELIEF study was to evaluate the efficacy and safety of two sequential intravenous (iv)/oral regimens: moxifloxacin iv/oral versus piperacillin/tazobactam (TZP) iv followed by oral amoxicillin/clavulanate (AMC).
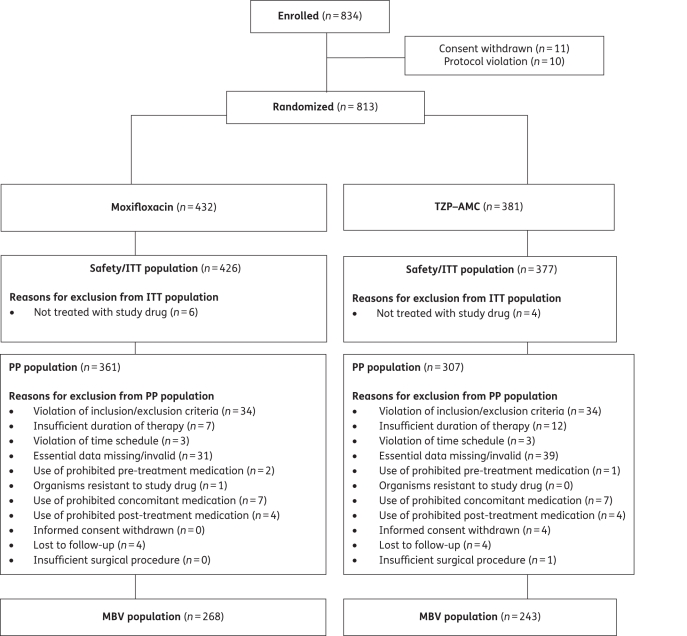
Patients and methods: The study had a prospective, randomized, double-dummy, double-blind, multicentre design. Patients ≥18 years were prospectively stratified according to complicated skin and skin structure infection (cSSSI) subtype/diagnosis (major abscess, diabetic foot infection, wound infection or infected ischaemic ulcer), surgical intervention and severity of illness. Diagnoses and disease severity were based on predetermined criteria, documented by repeated photographs, and confirmed by an independent data review committee. Patients were randomized to receive either 400 mg of moxifloxacin iv once daily followed by 400 mg of moxifloxacin orally once daily or 4.0/0.5 g of TZP iv thrice daily followed by 875/125 mg of AMC orally twice daily for 7-21 days. The primary efficacy variable was clinical response at test of cure (TOC) for the per-protocol (PP) population. Clinical efficacy was assessed by the data review committee based on repeated photographs and case descriptions. Clinical trials registry number: NCT 00402727.
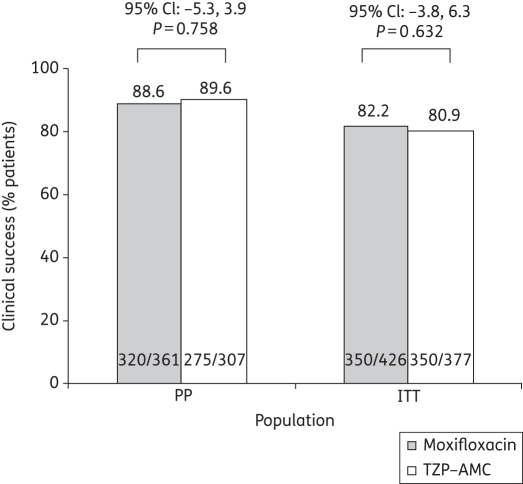
Results: A total of 813 patients were randomized. Clinical success rates at TOC were similar for moxifloxacin and TZP-AMC in the PP [320/361 (88.6%) versus 275/307 (89.6%), respectively; P = 0.758] and intent-to-treat (ITT) [350/426 (82.2%) versus 305/377 (80.9%), respectively; P = 0.632] populations. Thus, moxifloxacin was non-inferior to TZP-AMC. Bacteriological success rates were high in both treatment arms [moxifloxacin: 432/497 (86.9%) versus TZP-AMC: 370/429 (86.2%), microbiologically valid (MBV) population]. Moxifloxacin was non-inferior to TZP-AMC at TOC in both the MBV and the ITT populations. Both treatments were well tolerated.
Conclusions: Once-daily iv/oral moxifloxacin monotherapy was clinically and bacteriologically non-inferior to iv TZP thrice daily followed by oral AMC twice daily in patients with cSSSIs.
Trial registration: ClinicalTrials.gov NCT00402727.
Figures
References
-
- DiNubile MJ, Lipsky BA. Complicated infections of skin and skin structures: when the infection is more than skin deep. J Antimicrob Chemother. 2004;53(Suppl S2):ii37–50. doi:10.1093/jac/dkh202. - DOI - PubMed
-
- CDC. Soft tissue infections among injection drug users – San Francisco, California, 1996–2000. MMWR. 2001;50:381–4. - PubMed
-
- Giordano P, Song J, Pertel P, et al. Sequential intravenous/oral moxifloxacin versus intravenous piperacillin–tazobactam followed by oral amoxicillin–clavulanate for the treatment of complicated skin and skin structure infection. Int J Antimicrob Agents. 2005;26:357–65. doi:10.1016/j.ijantimicag.2005.07.017. - DOI - PubMed
-
- Nichols RL. Optimal treatment of complicated skin and skin structure infections. J Antimicrob Chemother. 1999;44:19–23. doi:10.1093/jac/44.suppl_1.19. - DOI - PubMed
-
- Lipsky BA, Weigelt JA, Gupta V, et al. Skin, soft tissue, bone, and joint infections in hospitalized patients: epidemiology and microbiological, clinical, and economic outcomes. J Antimicrob Chemother. 2007;60:370–6. doi:10.1093/jac/dkm130. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
