

Effectiveness of adenoidectomy in children with recurrent upper respiratory tract infections: open randomised controlled trial
- PMID: 21896611
- PMCID: PMC3167877
- DOI: 10.1136/bmj.d5154
Effectiveness of adenoidectomy in children with recurrent upper respiratory tract infections: open randomised controlled trial
Abstract
Objective: To assess the effectiveness of adenoidectomy in children with recurrent upper respiratory tract infections.
Design: Open randomised controlled trial.
Setting: 11 general hospitals and two academic centres.
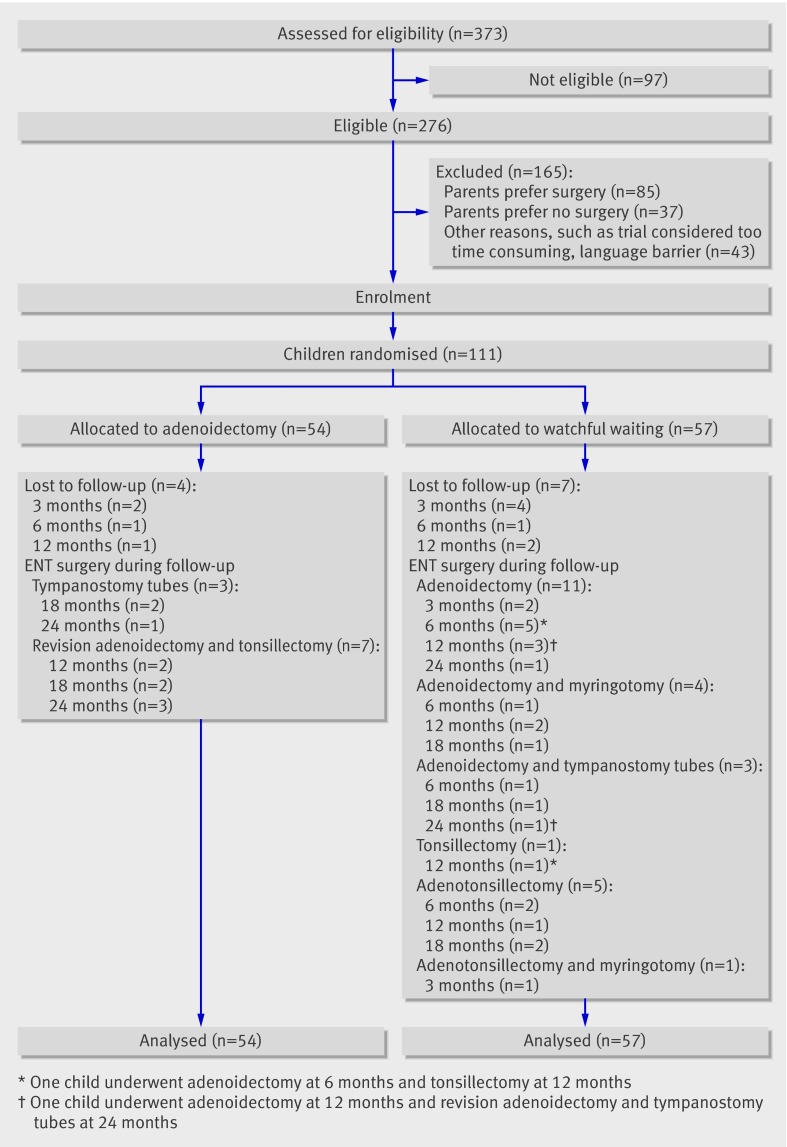
Participants: 111 children aged 1-6 with recurrent upper respiratory tract infections selected for adenoidectomy.
Intervention: A strategy of immediate adenoidectomy with or without myringotomy or a strategy of initial watchful waiting. Main outcome measure Primary outcome measure: number of upper respiratory tract infections per person year calculated from data obtained during the total follow-up (maximum 24 months).
Secondary outcome measures: days with upper respiratory tract infection per person year, middle ear complaints with fever in episodes and days, days with fever, prevalence of upper respiratory tract infections, and health related quality of life.
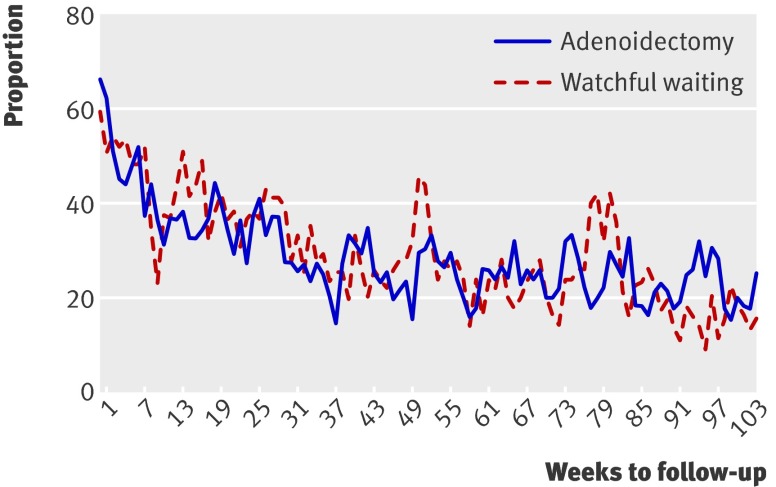
Results: During the median follow-up of 24 months, there were 7.91 episodes of upper respiratory tract infections per person year in the adenoidectomy group and 7.84 in the watchful waiting group (difference in incidence rate 0.07, 95% confidence interval -0.70 to 0.85). No relevant differences were found for days of upper respiratory tract infections and middle ear complaints with fever in episodes and days, nor for health related quality of life. The prevalence of upper respiratory tract infections decreased over time in both groups. Children in the adenoidectomy group had significantly more days with fever than the children in the watchful waiting group. Two children had complications related to surgery.
Conclusion: In children selected for adenoidectomy for recurrent upper respiratory tract infections, a strategy of immediate surgery confers no clinical benefits over a strategy of initial watchful waiting. Trial registration Dutch Trial Register NTR968: ISRCTN03720485.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Adenoidectomy in children with recurrent upper respiratory infections.BMJ. 2011 Sep 6;343:d5274. doi: 10.1136/bmj.d5274. BMJ. 2011. PMID: 21896612 No abstract available.
-
Adenoidectomy results in no benefit for children with recurrent upper respiratory tract infections.J Pediatr. 2012 Mar;160(3):526. doi: 10.1016/j.jpeds.2012.01.003. J Pediatr. 2012. PMID: 22329876 No abstract available.
References
-
- Nationaal Kompas Volksgezondheid. 2010. www.nationaalkompas.nl/gezondheid-en-ziekte/ziekten-en-aandoeningen/adem....
-
- Carabin H, Gyorkos TW, Soto JC, Penrod J, Joseph L, Collet JP. Estimation of direct and indirect costs because of common infections in toddlers attending day care centers. Pediatrics 1999;103:556-64. - PubMed
-
- Dixon RE. Economic costs of respiratory tract infections in the United States. Am J Med 1985;78:45-51. - PubMed
-
- Harsten G, Prellner K, Heldrup J, Kalm O, Kornfalt R. Acute respiratory tract infections in children. A three-year follow-up from birth. Acta Paediatr Scand 1990;79:402-9. - PubMed
-
- Haapkyla J, Karevold G, Kvaerner KJ, Pitkaranta A. Trends in otitis media surgery: a decrease in adenoidectomy. Int J Pediatr Otorhinolaryngol 2008;72:1207-13. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical