

Pharmacokinetic mismatch does not lead to emergence of isoniazid- or rifampin-resistant Mycobacterium tuberculosis but to better antimicrobial effect: a new paradigm for antituberculosis drug scheduling
- PMID: 21896907
- PMCID: PMC3195047
- DOI: 10.1128/AAC.00269-11
Pharmacokinetic mismatch does not lead to emergence of isoniazid- or rifampin-resistant Mycobacterium tuberculosis but to better antimicrobial effect: a new paradigm for antituberculosis drug scheduling
Abstract
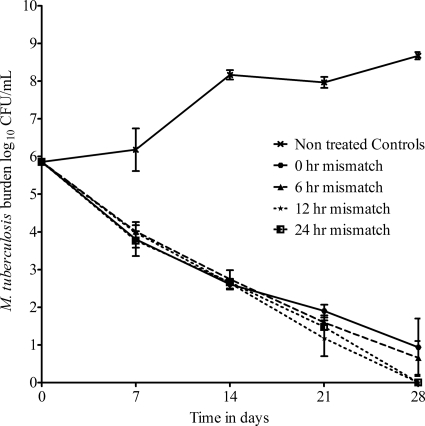
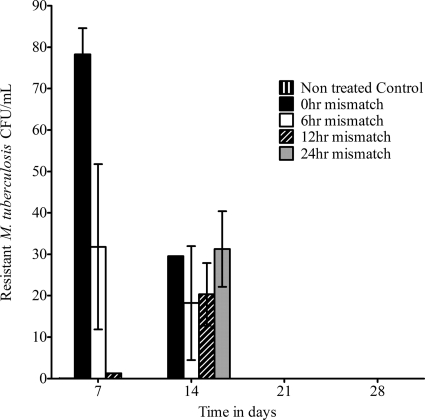
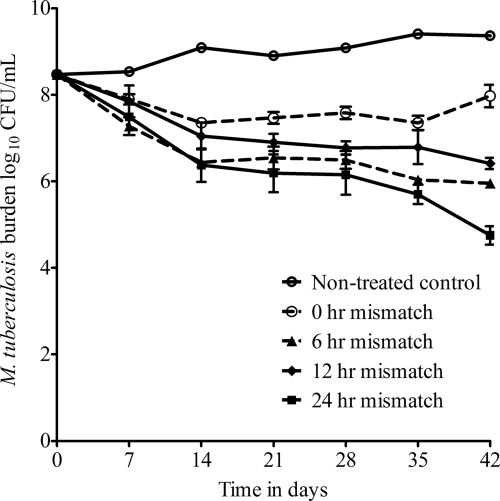
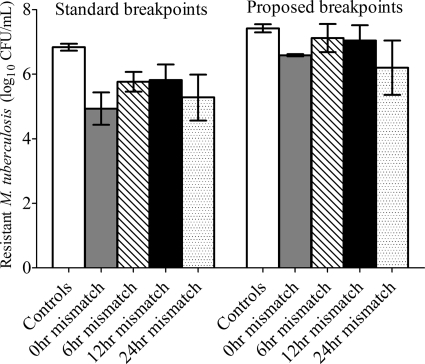
Multidrug resistant-tuberculosis is a pressing problem. One of the major mechanisms proposed to lead to the emergence of drug resistance is pharmacokinetic mismatch. Stated as a falsifiable hypothesis, the greater the pharmacokinetic mismatch between rifampin and isoniazid, the higher the isoniazid- and rifampin-resistant subpopulation sizes become with time. To test this, we performed hollow-fiber-system studies for both bactericidal and sterilizing effects in experiments of up to 42 days. We mimicked pharmacokinetics of 600-mg/day rifampin and 300-mg/day isoniazid administered to patients. Rifampin was administered first, followed by isoniazid 0, 6, 12, and 24 h later. The treatment was for drug-susceptible Mycobacterium tuberculosis in some experiments and hollow fiber systems with inoculum preseeded with isoniazid- and rifampin-resistant isogenic Mycobacterium tuberculosis strains in others. Analysis of variance revealed that the 12-h and 24-h-mismatched regimens always killed better than the matched regimens during both bactericidal and sterilizing effects (P < 0.05). This means that either the order of scheduling or the sequential administration of drugs in combination therapy may lead to significant improvement in microbial killing. Rifampin-resistant and isoniazid-resistant subpopulations were not significantly higher with increased mismatching in numerous analysis-of-variance comparisons. Thus, the pharmacokinetic mismatch hypothesis was rejected. Instead, sequential administration of anti-tuberculosis (TB) drugs (i.e., deliberate mismatch) following particular schedules suggests a new paradigm for accelerating M. tuberculosis killing. We conclude that current efforts aimed at better pharmacokinetic matching to decrease M. tuberculosis resistance emergence are likely futile and counterproductive.
Figures
Comment in
-
Pharmacokinetic mismatch of tuberculosis drugs.Antimicrob Agents Chemother. 2012 Mar;56(3):1666; author reply 1667. doi: 10.1128/AAC.06303-11. Antimicrob Agents Chemother. 2012. PMID: 22337897 Free PMC article. No abstract available.
References
-
- Ahmad Z., et al. 2009. Biphasic kill curve of isoniazid reveals the presence of drug-tolerant, not drug-resistant, Mycobacterium tuberculosis in the guinea pig. J. Infect. Dis. 200:1136–1143 - PubMed
-
- Bangsberg D. R., et al. 2006. Adherence-resistance relationships for protease and non-nucleoside reverse transcriptase inhibitors explained by virological fitness. AIDS 20:223–231 - PubMed
-
- Bangsberg D. R., Kroetz D. L., Deeks S. G. 2007. Adherence-resistance relationships to combination HIV antiretroviral therapy. Curr. HIV/AIDS Rep. 4:65–72 - PubMed
-
- Benator D., et al. 2002. Rifapentine and isoniazid once a week versus rifampicin and isoniazid twice a week for treatment of drug-susceptible pulmonary tuberculosis in HIV-negative patients: a randomised clinical trial. Lancet 360:528–534 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
