

Systemic sclerosis and the heart: current diagnosis and management
- PMID: 21897256
- PMCID: PMC3678364
- DOI: 10.1097/BOR.0b013e32834b8975
Systemic sclerosis and the heart: current diagnosis and management
Abstract
Purpose of review: When present clinically, cardiac involvement in systemic sclerosis (SSc) is a major risk factor for death. It is therefore vitally important to understand the epidemiology, screening, diagnosis, and treatment of the cardiac manifestations of SSc.
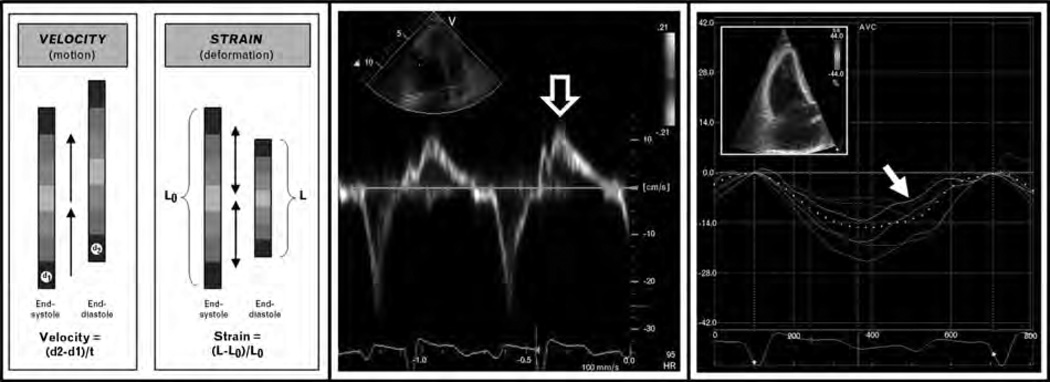
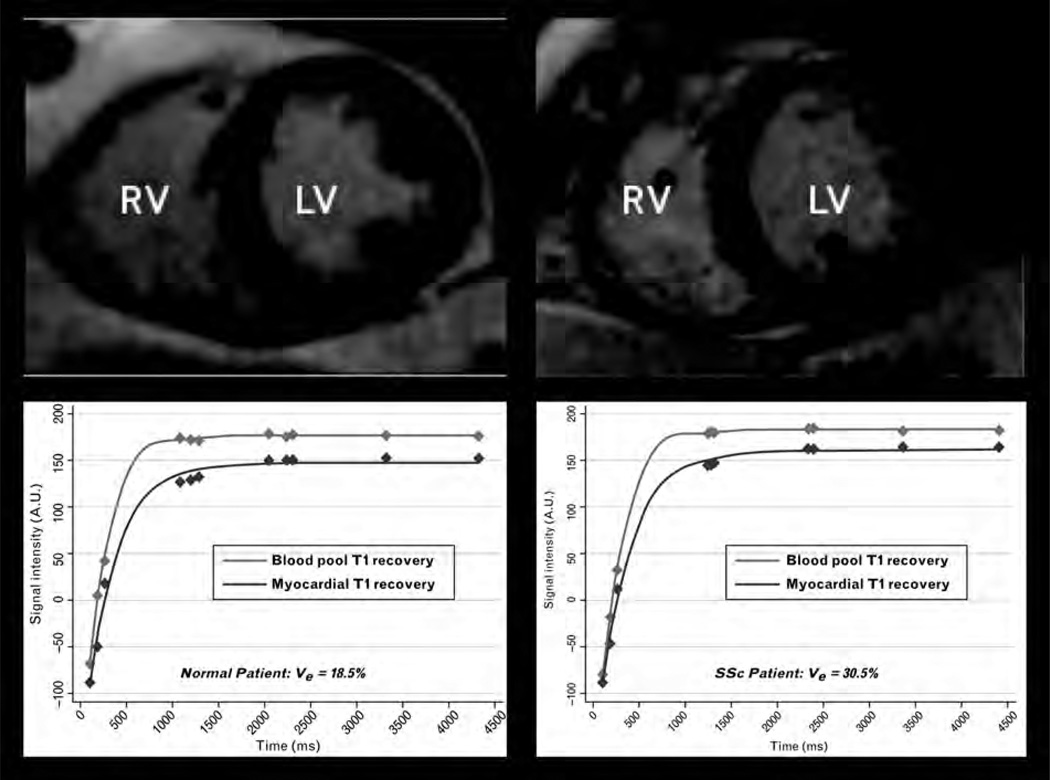
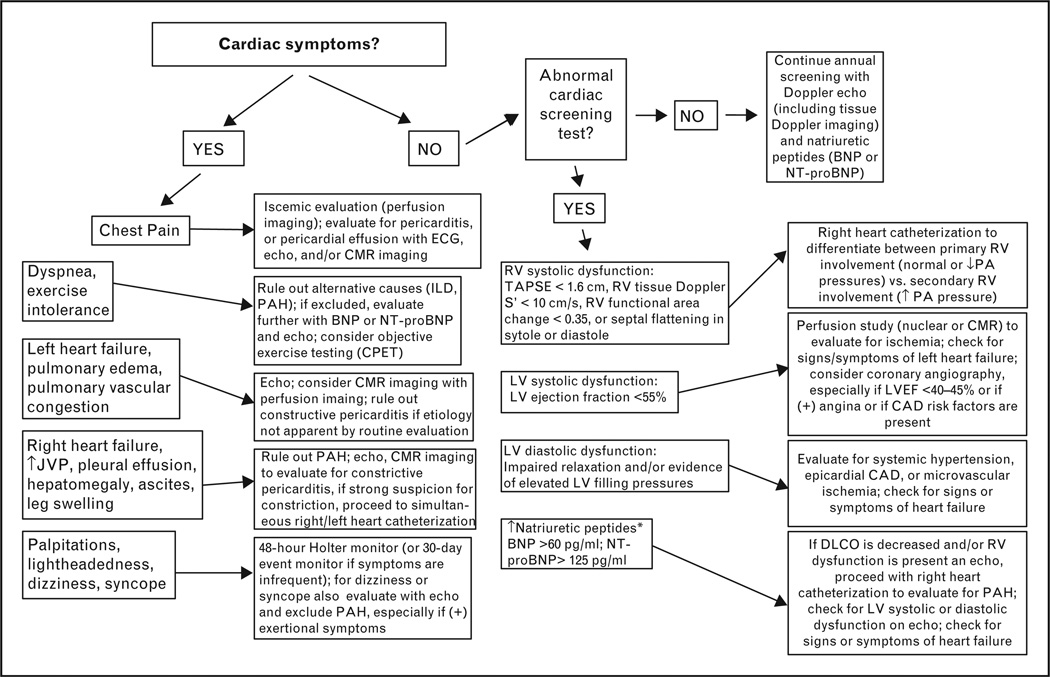
Recent findings: The epidemiology of cardiac involvement in SSc has been the subject of several recent studies. Most importantly, the prevalence of overt left ventricular (LV) systolic dysfunction and its associated risk factors have been defined, and patients with diffuse cutaneous SSc appear to be most susceptible to direct cardiac involvement. From a diagnostic and screening standpoint, tissue Doppler echocardiography and natriuretic peptides have provided fresh insight into subclinical cardiac dysfunction in SSc. Newer techniques, such as speckle-tracking echocardiography, diffuse myocardial fibrosis imaging, and absolute myocardial perfusion imaging, are poised to further advance our knowledge. Lastly, there is now consistent observational data to suggest a central role for calcium channel blockers in the treatment of microvascular ischemia and prevention of overt LV systolic dysfunction, although randomized controlled trials are lacking.
Summary: Recent studies have improved our understanding of cardiac involvement in SSc. Nevertheless, key questions regarding screening, diagnosis, and treatment remain. Novel diagnostic techniques and multicenter studies should yield important new data, which will hopefully ultimately result in improved outcomes.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Cardiac troponin T and NT-proBNP as diagnostic and prognostic biomarkers of primary cardiac involvement and disease severity in systemic sclerosis: A prospective study.Eur J Intern Med. 2019 Feb;60:46-53. doi: 10.1016/j.ejim.2018.10.013. Epub 2018 Oct 23. Eur J Intern Med. 2019. PMID: 30366614
-
Role of N-terminal pro-brain natriuretic peptide in detecting clinically significant cardiac involvement in systemic sclerosis patients.Clin Exp Rheumatol. 2012 Mar-Apr;30(2 Suppl 71):S81-5. Epub 2012 May 29. Clin Exp Rheumatol. 2012. PMID: 22691215
-
Systemic sclerosis and cardiac dysfunction: evolving concepts and diagnostic methodologies.Curr Opin Rheumatol. 2008 Nov;20(6):697-702. doi: 10.1097/BOR.0b013e328313bcf1. Curr Opin Rheumatol. 2008. PMID: 18946331 Review.
-
Early detection of cardiac involvement in systemic sclerosis assessed by tissue-Doppler echocardiography: relationship with neurohormonal activation and endothelial dysfunction.J Rheumatol. 2010 May;37(5):993-9. doi: 10.3899/jrheum.090931. Epub 2010 Mar 1. J Rheumatol. 2010. PMID: 20194451
-
Cardiac complications of systemic sclerosis and management: recent progress.Curr Opin Rheumatol. 2017 Nov;29(6):574-584. doi: 10.1097/BOR.0000000000000439. Curr Opin Rheumatol. 2017. PMID: 28957839 Review.
Cited by
-
Contractile reserve in systemic sclerosis patients as a major predictor of global cardiac impairment and exercise tolerance.Int J Cardiovasc Imaging. 2015 Mar;31(3):529-36. doi: 10.1007/s10554-014-0583-9. Epub 2014 Dec 30. Int J Cardiovasc Imaging. 2015. PMID: 25547289
-
Association of Systemic Sclerosis and Periodontitis with Vitamin D Levels.Nutrients. 2021 Feb 23;13(2):705. doi: 10.3390/nu13020705. Nutrients. 2021. PMID: 33672176 Free PMC article.
-
Assessment of Neutrophil-Lymphocyte Ratio and Systemic Immune-Inflammation Index in Systemic Scleroderma Patients with Focus on Cardiopulmonary Manifestations.Curr Health Sci J. 2024 Jul-Sep;50(3):421-427. doi: 10.12865/CHSJ.50.03.09. Epub 2024 Sep 30. Curr Health Sci J. 2024. PMID: 39574823 Free PMC article.
-
Cardiac Magnetic Resonance in Rheumatology to Detect Cardiac Involvement Since Early and Pre-clinical Stages of the Autoimmune Diseases: A Narrative Review.Front Cardiovasc Med. 2022 Jul 13;9:870200. doi: 10.3389/fcvm.2022.870200. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35911548 Free PMC article. Review.
-
The Role of the Multidisciplinary Health Care Team in the Management of Patients with Systemic Sclerosis.J Multidiscip Healthc. 2022 Apr 20;15:815-824. doi: 10.2147/JMDH.S295478. eCollection 2022. J Multidiscip Healthc. 2022. PMID: 35480063 Free PMC article. Review.
References
-
- Meune C, Vignaux O, Kahan A, et al. Heart involvement in systemic sclerosis: evolving concept and diagnostic methodologies. Arch Cardiovasc Dis. 2010;103:46–52. - PubMed
-
- Kahan A, Coghlan G, McLaughlin V. Cardiac complications of systemic sclerosis. Rheumatology (Oxford) 2009;48(Suppl 3):iii45–iii48. - PubMed
-
- Shah SJ, Kahan A. Cardiac involvement: evaluation and management. In: Varga J, Denton C, Wigley F, editors. Scleroderma: from pathogenesis to comprehensive management. New York: Springer; 2011.
-
-
Allanore Y, Meune C, Vonk MC, et al. Prevalence and factors associated with left ventricular dysfunction in the EULAR Scleroderma Trial and Research group (EUSTAR) database of patients with systemic sclerosis. Ann Rheum Dis. 2010;69:218–221.This is the largest study thus far of LV systolic dysfunction in SSc. The authors found a prevalence of 5.4% (defined as LV ejection fraction < 55%) and identified several factors associated with LV systolic dysfunction. Importantly, the authors found that calcium channel blocker usewas associated with reduced risk of LV systolic dysfunction.
-
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
