Endotracheal tube cuff pressure monitoring during neurosurgery - Manual vs. automatic method
- PMID: 21897508
- PMCID: PMC3161462
- DOI: 10.4103/0970-9185.83682
Endotracheal tube cuff pressure monitoring during neurosurgery - Manual vs. automatic method
Abstract
Background: Inflation and assessment of the endotracheal tube cuff pressure is often not appreciated as a critical aspect of endotracheal intubation. Appropriate endotracheal tube cuff pressure, endotracheal intubation seals the airway to prevent aspiration and provides for positive-pressure ventilation without air leak.
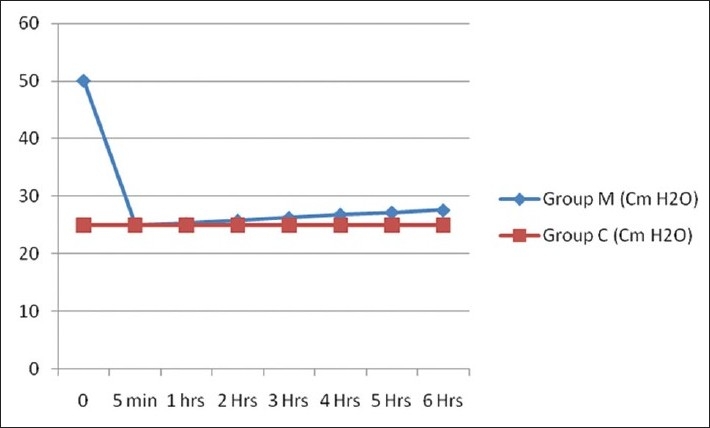
Materials and methods: Correlations between manual methods of assessing the pressure by an experienced anesthesiologists and assessment with maintenance of the pressure within the normal range by the automated pressure controller device were studied in 100 patients divided into two groups. In Group M, endotracheal tube cuff was inflated manually by a trained anesthesiologist and checked for its pressure hourly by cuff pressure monitor till the end of surgery. In Group C, endotracheal tube cuff was inflated by automated cuff pressure controller and pressure was maintained at 25-cm H(2)O throughout the surgeries. Repeated measure ANOVA was applied.
Results: Repeated measure ANOVA results showed that average of endotracheal tube cuff pressure of 50 patients taken at seven different points is significantly different (F-value: 171.102, P-value: 0.000). Bonferroni correction test shows that average of endotracheal tube cuff pressure in all six groups are significantly different from constant group (P = 0.000). No case of laryngomalacia, tracheomalacia, tracheal stenosis, tracheoesophageal fistula or aspiration pneumonitis was observed.
Conclusions: Endotracheal tube cuff pressure was significantly high when endotracheal tube cuff was inflated manually. The known complications of high endotracheal tube cuff pressure can be avoided if the cuff pressure controller device is used and manual methods cannot be relied upon for keeping the pressure within the recommended levels.
Keywords: Automatic cuff pressure controller; endotracheal tube cuff pressure; manual method; neurosurgery.
Conflict of interest statement
Figures
Similar articles
-
[Analysis on risk factors of endotracheal cuff under inflation in mechanically ventilated patients].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2014 Dec;26(12):870-4. doi: 10.3760/cma.j.issn.2095-4352.2014.12.005. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2014. PMID: 25476078 Chinese.
-
Assessment of aspiration risk from dynamic modulation of endotracheal tube cuff pressure.Laryngoscope. 2014 Jun;124(6):1415-9. doi: 10.1002/lary.24481. Epub 2013 Dec 9. Laryngoscope. 2014. PMID: 24155094
-
Is sealing cuff pressure, easy, reliable and safe technique for endotracheal tube cuff inflation?: A comparative study.Saudi J Anaesth. 2011 Apr;5(2):185-9. doi: 10.4103/1658-354X.82795. Saudi J Anaesth. 2011. PMID: 21804801 Free PMC article.
-
Problems Related to Endotracheal Intubation as an Input for the Design of a New Endotracheal Tube.Med Devices (Auckl). 2024 Oct 24;17:349-367. doi: 10.2147/MDER.S475964. eCollection 2024. Med Devices (Auckl). 2024. PMID: 39469419 Free PMC article. Review.
-
Endotracheal Tube Fallout in a Patient with Severe Obesity During Eye Surgery.2023 Mar 29. In: WebM&M: Case Studies [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2019 Oct 30–. 2023 Mar 29. In: WebM&M: Case Studies [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2019 Oct 30–. PMID: 40106638 Free Books & Documents. Review. No abstract available.
Cited by
-
Endotracheal cuff pressures in the PICU: Incidence of underinflation and overinflation.Can J Respir Ther. 2020 Jan 21;56:1-4. doi: 10.29390/cjrt-2019-018. eCollection 2019. Can J Respir Ther. 2020. PMID: 32095499 Free PMC article.
-
Tracheal tube cuff inflation guided by pressure volume loop closure associated with lower postoperative cuff-related complications: Prospective, randomized clinical trial.Saudi J Anaesth. 2014 Jul;8(3):328-34. doi: 10.4103/1658-354X.136422. Saudi J Anaesth. 2014. PMID: 25191181 Free PMC article.
-
A prospective observational study on changes in endo-tracheal tube cuff pressure and its correlation with airway pressures during various stages of robotic pelvic surgeries.J Anaesthesiol Clin Pharmacol. 2022 Apr-Jun;38(2):270-274. doi: 10.4103/joacp.JOACP_325_20. Epub 2022 Jul 28. J Anaesthesiol Clin Pharmacol. 2022. PMID: 36171935 Free PMC article.
-
Does endo-tracheal tube clamping prevent air leaks and maintain positive end-expiratory pressure during the switching of a ventilator in a patient in an intensive care unit? A bench study.PLoS One. 2020 Mar 11;15(3):e0230147. doi: 10.1371/journal.pone.0230147. eCollection 2020. PLoS One. 2020. PMID: 32160252 Free PMC article.
-
Effect of Tracheal Suctioning on Cuff Pressure in Mechanically Ventilated Patients: a Quasi-Experimental Study.Tanaffos. 2021 Jan;20(1):22-28. Tanaffos. 2021. PMID: 34394366 Free PMC article.
References
-
- Dullenkopf A, Gerber A, Weiss M. Fluid leakage past tracheal tube cuffs: Evaluation of the new Microcuff endotracheal tube. Intensive Care Med. 2003;29:1849–53. - PubMed
-
- Lien TC, Wang JH. Incidence of pulmonary aspiration with different kinds of artificial airways. Zhonghua Yi Xue Za Zhi (Taipei) 1992;49:348–53. - PubMed
-
- Bernhard WN, Yost L, Joynes D, Cothalis S, Turndorf H. Intracuff pressures in endotracheal and tracheostomy tubes.Related cuff physical characteristics. Chest. 1985;87:720–5. - PubMed
-
- Parwani V, Hahn I, Hsu B, Hoffman R. Experienced emergency physicians cannot safely or accurately inflate endotracheal tube cuffs or estimate endotracheal tube cuff pressure using standard technique [abstract] Acad Emerg Med. 2004;11:490. - PubMed
-
- Mandoe H, Nikolajsen L, Lintrup U, Jepsen D, Molgaard J. Sore throat after endotracheal intubation. Anesth Analg. 1992;74:897–900. - PubMed