

Practice Guideline
doi: 10.1002/hep.24641.
Epub 2011 Sep 26.
An update on treatment of genotype 1 chronic hepatitis C virus infection: 2011 practice guideline by the American Association for the Study of Liver Diseases
Affiliations
- PMID: 21898493
- PMCID: PMC3229841
- DOI: 10.1002/hep.24641
Item in Clipboard
Practice Guideline
An update on treatment of genotype 1 chronic hepatitis C virus infection: 2011 practice guideline by the American Association for the Study of Liver Diseases
Hepatology.
2011 Oct.
Free PMC article
No abstract available
Figures
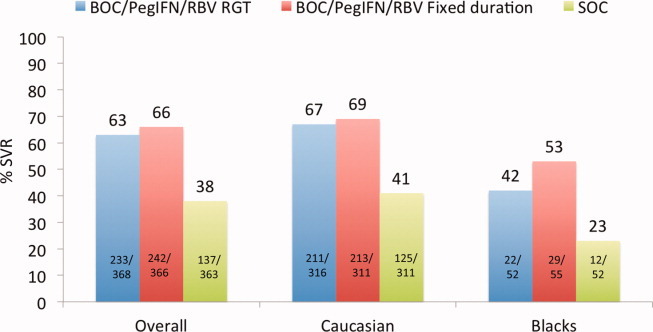
Sustained virological response (SVR) rates, overall and according to race, in treatment-naïve patients with genotype 1 chronic HCV infection: Boceprevir (BOC) plus peginterferon (PegIFN) and ribavirin (RBV) versus standard of care (SOC). All patients were first treated with PegIFN + RBV for 4 weeks as lead-in therapy followed by one of three regiments: (1) BOC/PegIFN/RBV RGT - triple therapy for 24 weeks provided HCV RNA levels were negative weeks 8 thorugh 24 – response guided therapy; those with a detectable HCV RNA level between weeks 8 and 24 received SOC for an additional 20 weeks; (2) BOC/PegIFN/RBV fixed duration - triple therapy for a fixed duration of 44 weeks; and (3) SOC - consisted of PegIFN and weight based RBV administered for 48 weeks.
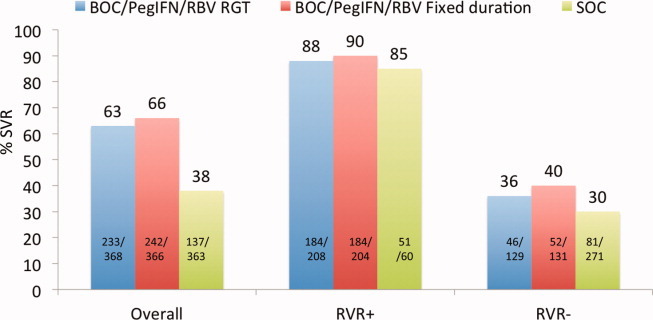
Sustained virological response (SVR) rates, overall and based on a rapid virological response (RVR, undetectable HCV RNA at week 8 [week 4 of triple therapy]) in treatment-naïve patients with genotype 1 chronic HCV infection: Boceprevir (BOC) plus peginterferon (PegIFN) versus standard of care (SOC). All patients were first treated with PegIFN + RBV for 4 weeks as lead-in therapy followed by one of three regiments: (1) BOC/PegIFN/RBV RGT - patients who achieved an RVR (undetable HCV RNA at week 8 [week 4 of triple therapy]) continued treatment for an additional 24 weeks (RGT - response guided therapy); if an RVR did not develop, treatment with triple therapy continued to week 28 followed by SOC treatment for 20 weeks. SOC treatment consisted of PegIFN and RBV administered for 48 weeks. Note that the combined numbers of RVR-positive and RVR-negative patients are not equivalent to the total number of patients enrolled, presumably because of missing HCV RNA values at the week 8 time point.
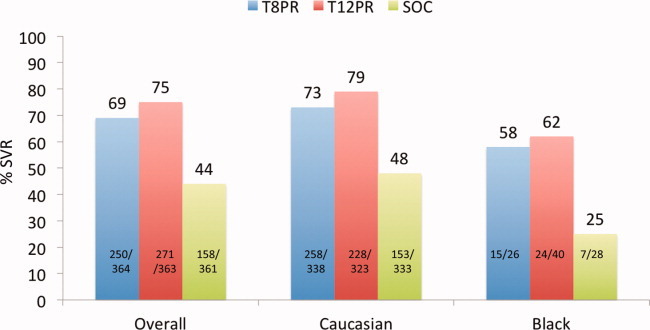
Sustained virological response (SVR) rates, overall and according to race, in treatment naïve patients with genotype 1 chronic HCV infection: Telaprevir (TVR) plus peginterferon and ribavirin (PR) treatment for 8 (T8PR) or 12 (T12PR) weeks versus standard of care (SOC). Patients in the triple therapy arms who developed an eRVR (extended rapid virological response; defined as undetectable HCV RNA at weeks 4 and 12) stopped treatment at week 24 (response-guided therapy, RGT); if eRVR did not develop, treatment continued to 48 weeks. SOC treatment consisted of PegIFN and RBV administered for 48 weeks.
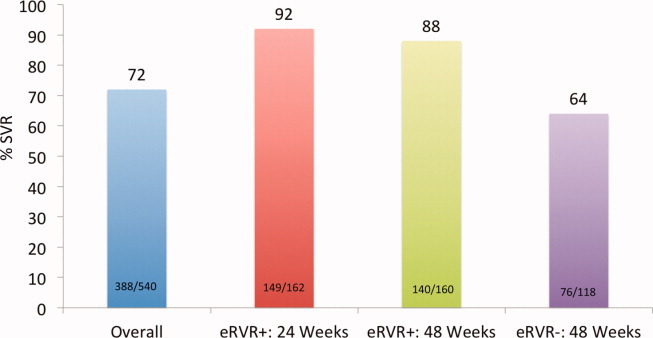
Sustained virological response (SVR) rates in treatment naïve patients with genotype 1 chronic HCV infection: Telaprevir (TVR) plus peginterferon and ribavirin (PR) results overall and among those who did or did not achieve an eRVR (extended rapid virological response; undetectable HCV RNA at weeks 4 and 12). Patients who achieved an eRVR were randomized at week 20 to receive an additional 4 or an additional 28 weeks of SOC therapy; those who did not develop an eRVR were not randomized and all received an additional 24 weeks of SOC therapy.
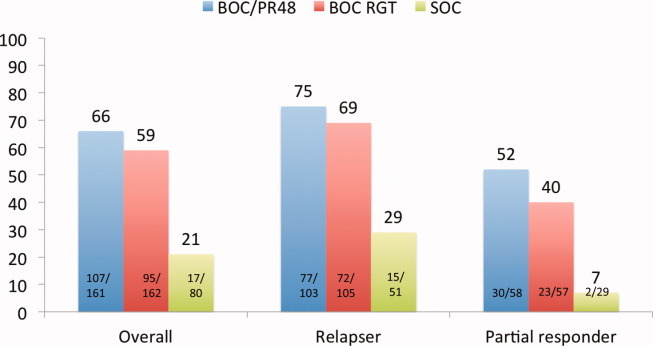
Sustained virological response (SVR) rates, overall and among relapsers and partial responders, in treatment experienced patients with genotype 1 chronic HCV infection: Boceprevir (BOC) plus peginterferon and ribavirin (PR) versus standard of care (SOC). All patients were first treated with PegIFN and RBV for 4 weeks as lead-in therapy followed by one of 3 regimens: (1) BOC/PR48 triple therapy for 44 weeks. (2) BOC RGT triple therapy for 32 weeks if an eRVR was achieved (undetecatble HCV RNA at week 8 and 12). If an eRVR was not achieved, but HCV RNA became undetectable at week 12, BOC was stopped at week 32 and patients received an additional 12 weeks of SOC treatment (total 48 weeks of therapy). (3) SOC treatment consisted of PegIFN and RBV administered for 48 weeks.
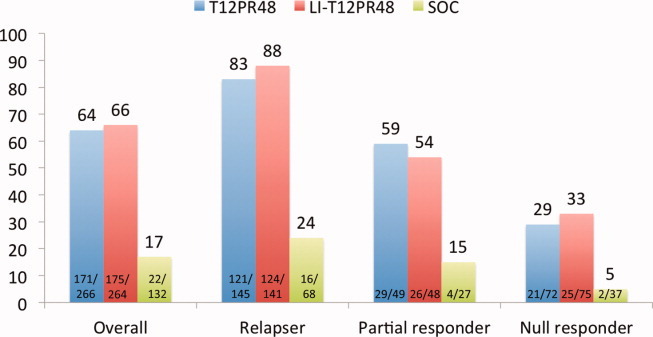
Sustained virological response (SVR) rates, overall and among relapsers, partial responders, and null responders, in treatment-experienced patients with genotype 1 chronic HCV infection. T12PR48: Telaprevir (TVR) plus peginterferon and ribavirin (PR) administered for 12 weeks followed by 36 PR for 12 weeks followed by PR for 32 weeks; SOC consisted of PegIFN and RBV administered for 48 weeks.
Comment in
-
Rapid virological response: is it four or eight weeks?Hepatology. 2012 Mar;55(3):979; author reply 980-1. doi: 10.1002/hep.25527. Hepatology. 2012. PMID: 22161760 No abstract available.
-
An update on treatment of hepatitis C virus genotype 1 infection and viral load assessments.Hepatology. 2012 Mar;55(3):979-80; author reply 980-1. doi: 10.1002/hep.25516. Hepatology. 2012. PMID: 22161994 No abstract available.
References
-
- Eddy D. A manual for assessing health practices and designing practice guidelines. Philadelphia: American College of Physicians; 1996.
-
- American Gastroenterological Association policy statement on the use of medical practice guidelines by managed care organizations and insurance carriers. Gastroenterology. 1995;108:925–926. - PubMed
-
- American Heart Association. 2011. http://my.americanheart.org/idc/groups/ahamah-public/@wcm/@sop/documents.... Accessed August.
-
- Shiffman RN, Shekelle P, Overhage JM, Slutsky J, Grimshaw J, Deshpande AM. Standardized reporting of clinical practice guidelines: a proposal from the Conference on Guideline Standardization. Ann Intern Med. 2003;139:493–498. - PubMed
-
- Manns MP, McHutchison JG, Gordon SC, Rustgi VK, Shiffman M, Reindollar R, et al. Peginterferon alfa-2b plus ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment of chronic hepatitis C: a randomised trial. Lancet. 2001;358:958–965. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources