

Stenting versus aggressive medical therapy for intracranial arterial stenosis
- PMID: 21899409
- PMCID: PMC3552515
- DOI: 10.1056/NEJMoa1105335
Stenting versus aggressive medical therapy for intracranial arterial stenosis
Erratum in
- N Engl J Med. 2012 Jul 5;367(1):93
Abstract
Background: Atherosclerotic intracranial arterial stenosis is an important cause of stroke that is increasingly being treated with percutaneous transluminal angioplasty and stenting (PTAS) to prevent recurrent stroke. However, PTAS has not been compared with medical management in a randomized trial.
Methods: We randomly assigned patients who had a recent transient ischemic attack or stroke attributed to stenosis of 70 to 99% of the diameter of a major intracranial artery to aggressive medical management alone or aggressive medical management plus PTAS with the use of the Wingspan stent system. The primary end point was stroke or death within 30 days after enrollment or after a revascularization procedure for the qualifying lesion during the follow-up period or stroke in the territory of the qualifying artery beyond 30 days.
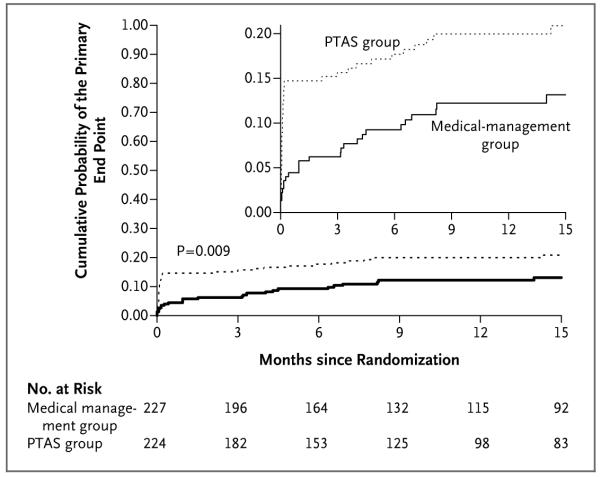
Results: Enrollment was stopped after 451 patients underwent randomization, because the 30-day rate of stroke or death was 14.7% in the PTAS group (nonfatal stroke, 12.5%; fatal stroke, 2.2%) and 5.8% in the medical-management group (nonfatal stroke, 5.3%; non-stroke-related death, 0.4%) (P=0.002). Beyond 30 days, stroke in the same territory occurred in 13 patients in each group. Currently, the mean duration of follow-up, which is ongoing, is 11.9 months. The probability of the occurrence of a primary end-point event over time differed significantly between the two treatment groups (P=0.009), with 1-year rates of the primary end point of 20.0% in the PTAS group and 12.2% in the medical-management group.
Conclusions: In patients with intracranial arterial stenosis, aggressive medical management was superior to PTAS with the use of the Wingspan stent system, both because the risk of early stroke after PTAS was high and because the risk of stroke with aggressive medical therapy alone was lower than expected. (Funded by the National Institute of Neurological Disorders and Stroke and others; SAMMPRIS ClinicalTrials.gov number, NCT00576693.).
Trial registration: ClinicalTrials.gov NCT00004732 NCT00059306 NCT00576693.
Figures
Comment in
-
The challenges of intracranial revascularization for stroke prevention.N Engl J Med. 2011 Sep 15;365(11):1054-5. doi: 10.1056/NEJMe1108394. Epub 2011 Sep 7. N Engl J Med. 2011. PMID: 21899410 No abstract available.
-
Stroke: new TIA definition, new anticoagulation, no stenting.J Neurol. 2011 Nov;258(11):2107-9. doi: 10.1007/s00415-011-6282-8. J Neurol. 2011. PMID: 22037951 No abstract available.
-
Comment on: Stenting versus aggressive medical therapy for intracranial arterial stenosis : Chimowitz MI, Lynn MJ, Derdeyn CP, et al. N Engl J Med. 2011;365:993-1003.Clin Neuroradiol. 2011 Nov;21(4):257-9. doi: 10.1007/s00062-011-0107-0. Clin Neuroradiol. 2011. PMID: 22071775 No abstract available.
-
Stenting versus medical therapy for intracranial arterial stenosis.N Engl J Med. 2011 Dec 1;365(22):2140; author reply 2141. doi: 10.1056/NEJMc1111906. N Engl J Med. 2011. PMID: 22129265 No abstract available.
-
Stenting versus medical therapy for intracranial arterial stenosis.N Engl J Med. 2011 Dec 1;365(22):2140-1; author reply 2141. doi: 10.1056/NEJMc1111906. N Engl J Med. 2011. PMID: 22129266 No abstract available.
-
[SAMMPRIS -- a look behind the scenes].Radiologe. 2012 Feb;52(2):105-6. doi: 10.1007/s00117-011-2275-y. Radiologe. 2012. PMID: 22349953 German. No abstract available.
-
In TIA or stroke patients with intracranial arterial stenosis, aggressive medical therapy was superior to percutaneous transluminal angioplasty and stenting for 30-day risk of further stroke or death.Evid Based Med. 2012 Aug;17(4):115-6. doi: 10.1136/ebmed-2011-100451. Epub 2012 Mar 7. Evid Based Med. 2012. PMID: 22398115 No abstract available.
-
Stenting versus aggressive medical therapy for intracranial arterial stenosis: more harm than good.Crit Care. 2012 May 9;16(3):310. doi: 10.1186/cc11326. Crit Care. 2012. PMID: 22574950 Free PMC article.
-
Is there a contribution of anesthesia to the outcome of the SAMMPRIS trial?Neurosurgery. 2014 Feb;74(2):E234-5. doi: 10.1227/NEU.0000000000000211. Neurosurgery. 2014. PMID: 24141483 No abstract available.
-
In reply: Is there a contribution of anesthesia to the outcome of the SAMMPRIS trial?Neurosurgery. 2014 Feb;74(2):E235-6. doi: 10.1227/NEU.0000000000000227. Neurosurgery. 2014. PMID: 24149979 Free PMC article. No abstract available.
References
-
- Wong LK. Global burden of intracranial atherosclerosis. Int J Stroke. 2006;1:158–9. - PubMed
-
- Gorelick PB, Wong KS, Bae HJ, Pandey DK. Large artery intracranial occlusive disease: a large worldwide burden but a relatively neglected frontier. Stroke. 2008;39:2396–9. - PubMed
-
- Arenillas JF. Intracranial atherosclerosis: current concepts. Stroke. 2011;42(Suppl):S20–S23. - PubMed
-
- Sacco RL, Kargman D, Gu Q, Zamanillo MC. Race-ethnicity and determinants of intracranial atherosclerotic cerebral infarction: the Northern Manhattan Stroke Study. Stroke. 1995;26:14–20. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical