

Association of unconscious race and social class bias with vignette-based clinical assessments by medical students
- PMID: 21900134
- PMCID: PMC3684149
- DOI: 10.1001/jama.2011.1248
Association of unconscious race and social class bias with vignette-based clinical assessments by medical students
Abstract
Context: Studies involving physicians suggest that unconscious bias may be related to clinical decision making and may predict poor patient-physician interaction. The presence of unconscious race and social class bias and its association with clinical assessments or decision making among medical students is unknown.
Objective: To estimate unconscious race and social class bias among first-year medical students and investigate its relationship with assessments made during clinical vignettes.
Design, setting, and participants: A secure Web-based survey was administered to 211 medical students entering classes at Johns Hopkins School of Medicine, Baltimore, Maryland, in August 2009 and August 2010. The survey included the Implicit Association Test (IAT) to assess unconscious preferences, direct questions regarding students' explicit race and social class preferences, and 8 clinical assessment vignettes focused on pain assessment, informed consent, patient reliability, and patient trust. Adjusting for student demographics, multiple logistic regression was used to determine whether responses to the vignettes were associated with unconscious race or social class preferences.
Main outcome measures: Association of scores on an established IAT for race and a novel IAT for social class with vignette responses.
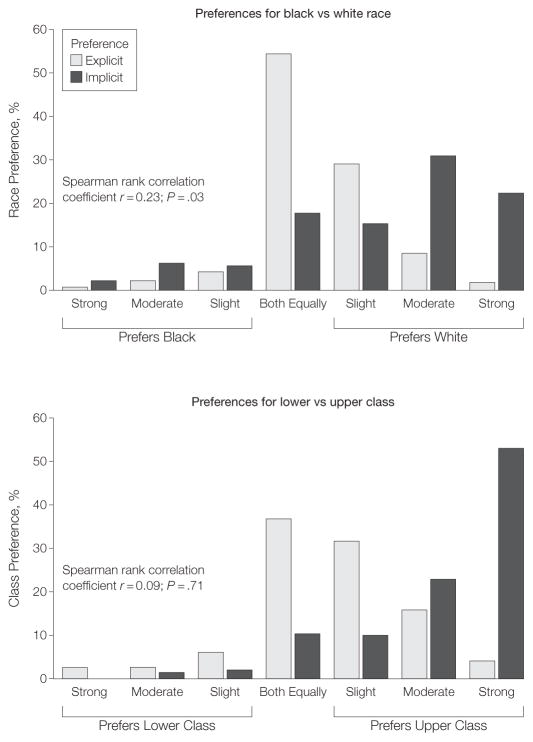
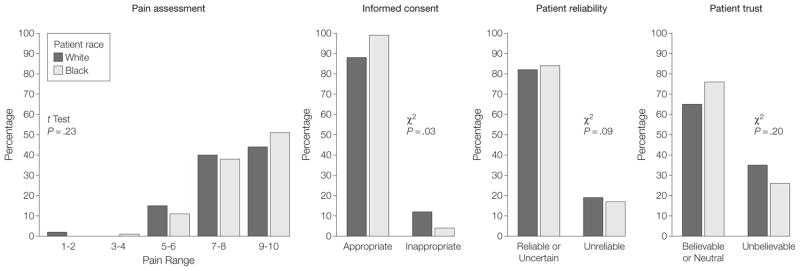
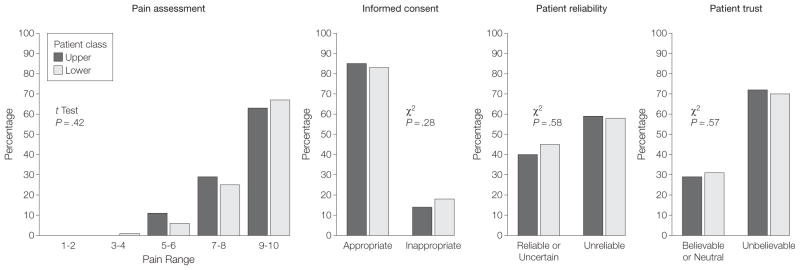
Results: Among the 202 students who completed the survey, IAT responses were consistent with an implicit preference toward white persons among 140 students (69%, 95% CI, 61%-75%). Responses were consistent with a preference toward those in the upper class among 174 students (86%, 95% CI, 80%-90%). Assessments generally did not vary by patient race or occupation, and multivariable analyses for all vignettes found no significant relationship between implicit biases and clinical assessments. Regression coefficient for the association between pain assessment and race IAT scores was -0.49 (95% CI, -1.00 to 0.03) and for social class, the coefficient was -0.04 (95% CI, -0.50 to 0.41). Adjusted odds ratios for other vignettes ranged from 0.69 to 3.03 per unit change in IAT score, but none were statistically significant. Analysis stratified by vignette patient race or class status yielded similarly negative results. Tests for interactions between patient race or class status and student IAT D scores in predicting clinical assessments were not statistically significant.
Conclusions: The majority of first-year medical students at a single school had IAT scores consistent with implicit preference for white persons and possibly for those in the upper class. However, overall vignette-based clinical assessments were not associated with patient race or occupation, and no association existed between implicit preferences and the assessments.
Conflict of interest statement
Figures
Comment in
-
Exploring unconscious bias in disparities research and medical education.JAMA. 2011 Sep 7;306(9):995-6. doi: 10.1001/jama.2011.1275. JAMA. 2011. PMID: 21900142 Free PMC article. No abstract available.
-
Unconscious race and social class bias in medical students.JAMA. 2011 Dec 14;306(22):2454; author reply 2454-5. doi: 10.1001/jama.2011.1770. JAMA. 2011. PMID: 22166602 No abstract available.
References
-
- Smedley BD, Stith AY, Nelson AR. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington, DC: National Academies Press; 2003. - PubMed
-
- Haider AH, Chang DC, Efron DT, Haut ER, Crandall M, Cornwell EE., III Race and insurance status as risk factors for trauma mortality. Arch Surg. 2008;143(10):945–949. - PubMed
-
- Haider AH, Efron DT, Haut ER, DiRusso SM, Sullivan T, Cornwell EE., III Black children experience worse clinical and functional outcomes after traumatic brain injury: an analysis of the National Pediatric Trauma Registry. J Trauma. 2007;62(5):1259–1262. - PubMed
-
- Crompton JG, Pollack KM, Oyetunji T, et al. Racial disparities in motorcycle-related mortality: an analysis of the National Trauma Data Bank. Am J Surg. 2010;200(2):191–196. - PubMed
