

Trauma exposure and posttraumatic stress disorder among employees of New York City companies affected by the September 11, 2001 attacks on the World Trade Center
- PMID: 21900416
- PMCID: PMC3842159
- DOI: 10.1001/dmp.2011.50
Trauma exposure and posttraumatic stress disorder among employees of New York City companies affected by the September 11, 2001 attacks on the World Trade Center
Abstract
Objective: Several studies have provided prevalence estimates of posttraumatic stress disorder (PTSD) related to the September 11, 2001 (9/11) attacks in broadly affected populations, although without sufficiently addressing qualifying exposures required for assessing PTSD and estimating its prevalence. A premise that people throughout the New York City area were exposed to the attacks on the World Trade Center (WTC) towers and are thus at risk for developing PTSD has important implications for both prevalence estimates and service provision. This premise has not, however, been tested with respect to DSM-IV-TR criteria for PTSD. This study examined associations between geographic distance from the 9/11 attacks on the WTC and reported 9/11 trauma exposures, and the role of specific trauma exposures in the development of PTSD.
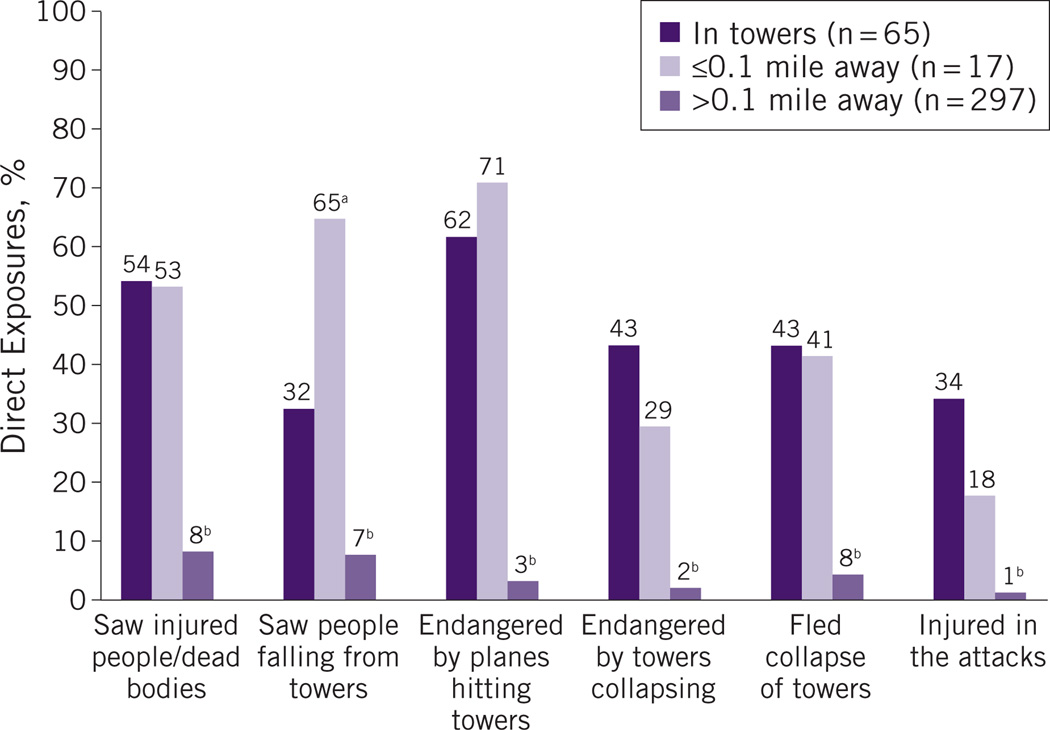
Methods: Approximately 3 years after the attacks, 379 surviving employees (102 with direct exposures, including 65 in the towers, and 277 with varied exposures) recruited from 8 affected organizations were interviewed using the Diagnostic Interview Schedule/Disaster Supplement and reassessed at 6 years. The estimated closest geographic distance from the WTC towers during the attacks and specific disaster exposures were compared with the development of 9/11-related PTSD as defined by the Diagnostic and Statistical Manual, Fourth Edition, Text Revision.
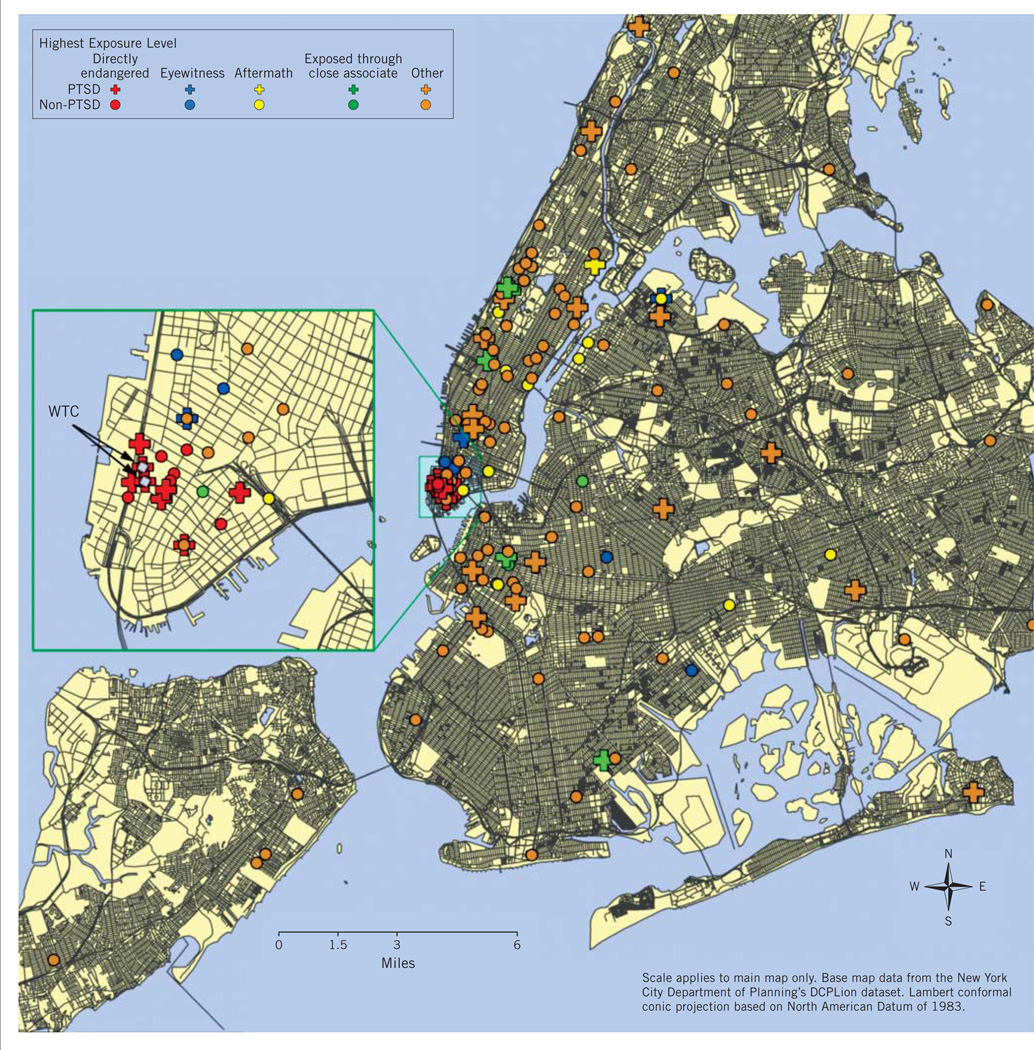
Results: The direct exposure zone was largely concentrated within a radius of 0.1 mi and completely contained within 0.75 mi of the towers. PTSD symptom criteria at any time after the disaster were met by 35% of people directly exposed to danger, 20% of those exposed only through witnessed experiences, and 35% of those exposed only through a close associate's direct exposure. Outside these exposure groups, few possible sources of exposure were evident among the few who were symptomatic, most of whom had preexisting psychiatric illness.
Conclusions: Exposures deserve careful consideration among widely affected populations after large terrorist attacks when conducting clinical assessments, estimating the magnitude of population PTSD burdens, and projecting needs for specific mental health interventions.
Conflict of interest statement
Figures
Comment in
-
Reexamining the role of the traumatic stressor and the trajectory of posttraumatic distress in the wake of disaster.Disaster Med Public Health Prep. 2011 Sep;5 Suppl 2:S172-5. doi: 10.1001/dmp.2011.51. Disaster Med Public Health Prep. 2011. PMID: 21908694 No abstract available.
References
-
- Silver RC, Holman A, McIntosh DN, et al. Coping with a national trauma: a nationwide longitudinal study of responses to the terrorist attacks of September 11. In: Neria Y, Gross R, Marshall RD, et al., editors. 9/11: Mental Health in the Wake of Terrorist Attacks. New York: Cambridge University Press; 2006. pp. 45–70.
-
- Galea S, Ahern J, Resnick H, et al. Psychological sequelae of the September 11 terrorist attacks in New York City. N Engl J Med. 2002;346(13):982–987. - PubMed
-
- Galea S, Vlahov D, Resnick H, et al. Trends of probable post-traumatic stress disorder in New York City after the September 11 terrorist attacks. Am J Epidemiol. 2003;158(6):514–524. - PubMed
-
- Schuster MA, Stein BD, Jaycox L, et al. A national survey of stress reactions after the September 11, 2001, terrorist attacks. N Engl J Med. 2001;345(20):1507–1512. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
