

Activation of ERBB2 signaling causes resistance to the EGFR-directed therapeutic antibody cetuximab
- PMID: 21900593
- PMCID: PMC3268675
- DOI: 10.1126/scitranslmed.3002442
Activation of ERBB2 signaling causes resistance to the EGFR-directed therapeutic antibody cetuximab
Abstract
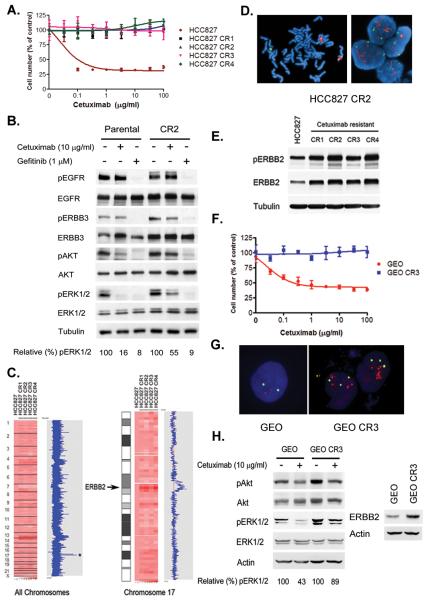
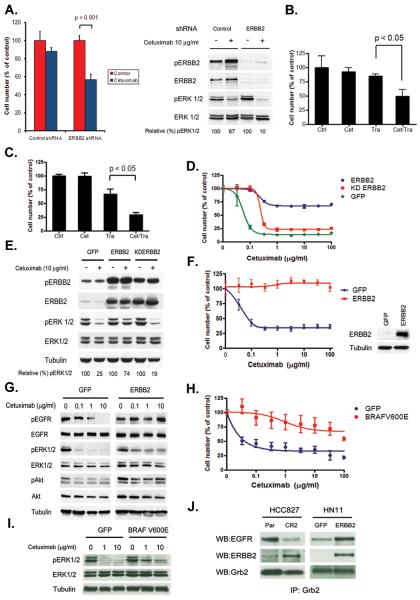
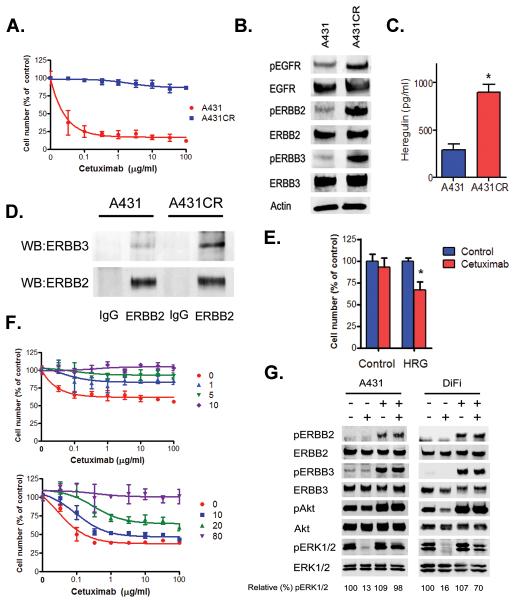
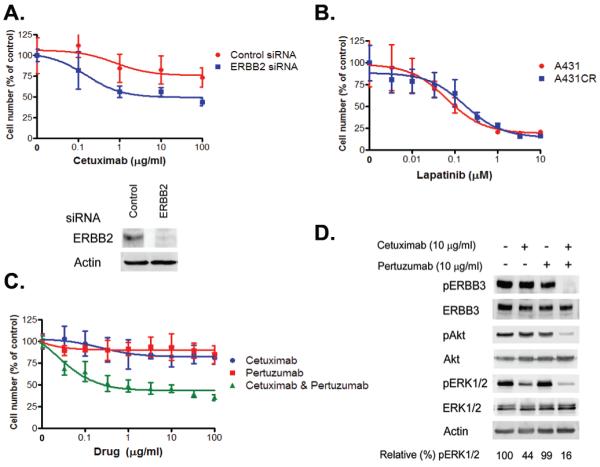
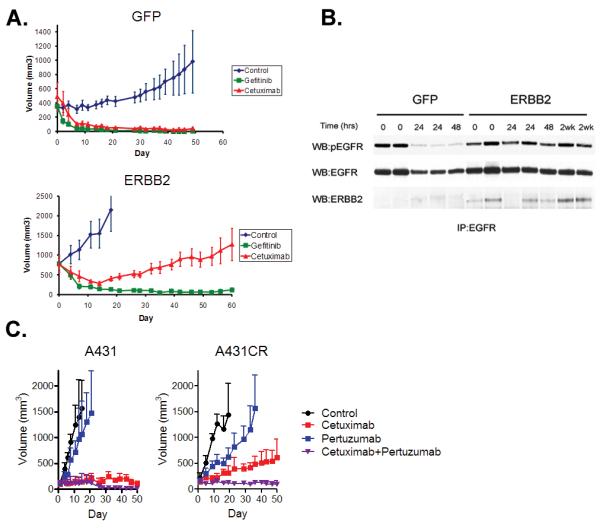
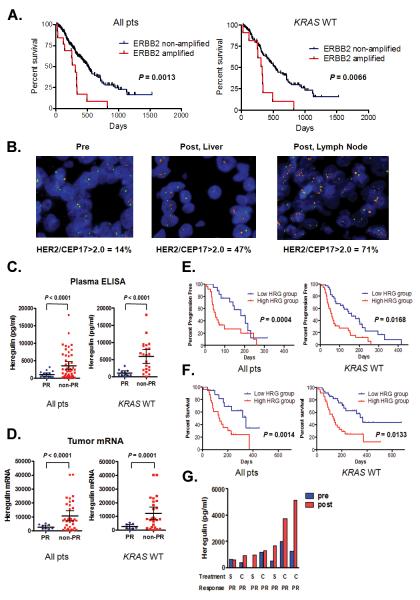
Cetuximab, an antibody directed against the epidermal growth factor receptor, is an effective clinical therapy for patients with colorectal, head and neck, and non-small cell lung cancer, particularly for those with KRAS and BRAF wild-type cancers. Treatment in all patients is limited eventually by the development of acquired resistance, but little is known about the underlying mechanism. Here, we show that activation of ERBB2 signaling in cell lines, either through ERBB2 amplification or through heregulin up-regulation, leads to persistent extracellular signal-regulated kinase 1/2 signaling and consequently to cetuximab resistance. Inhibition of ERBB2 or disruption of ERBB2/ERBB3 heterodimerization restores cetuximab sensitivity in vitro and in vivo. A subset of colorectal cancer patients who exhibit either de novo or acquired resistance to cetuximab-based therapy has ERBB2 amplification or high levels of circulating heregulin. Collectively, these findings identify two distinct resistance mechanisms, both of which promote aberrant ERBB2 signaling, that mediate cetuximab resistance. Moreover, these results suggest that ERBB2 inhibitors, in combination with cetuximab, represent a rational therapeutic strategy that should be assessed in patients with cetuximab-resistant cancers.
Figures
Comment in
-
Resistance: Cetuximab's tip to become irresistible.Nat Rev Clin Oncol. 2011 Sep 27;8(11):629. doi: 10.1038/nrclinonc.2011.145. Nat Rev Clin Oncol. 2011. PMID: 21946843 No abstract available.
-
Resistance to EGFR-targeted therapy: a family affair.Cancer Cell. 2011 Oct 18;20(4):423-5. doi: 10.1016/j.ccr.2011.10.006. Cancer Cell. 2011. PMID: 22014569 Free PMC article.
References
-
- Jonker DJ, O’Callaghan CJ, Karapetis CS, Zalcberg JR, Tu D, Au HJ, Berry SR, Krahn M, Price T, Simes RJ, Tebbutt NC, van Hazel G, Wierzbicki R, Langer C, Moore MJ. Cetuximab for the treatment of colorectal cancer. N Engl J Med. 2007;357:2040–2048. - PubMed
-
- Vermorken JB, Mesia R, Rivera F, Remenar E, Kawecki A, Rottey S, Erfan J, Zabolotnyy D, Kienzer HR, Cupissol D, Peyrade F, Benasso M, Vynnychenko I, De Raucourt D, Bokemeyer C, Schueler A, Amellal N, Hitt R. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N Engl J Med. 2008;359:1116–1127. - PubMed
-
- Pirker R, Pereira JR, Szczesna A, von Pawel J, Krzakowski M, Ramlau R, Vynnychenko I, Park K, Yu CT, Ganul V, Roh JK, Bajetta E, O’Byrne K, de Marinis F, Eberhardt W, Goddemeier T, Emig M, Gatzemeier U. Cetuximab plus chemotherapy in patients with advanced non-small-cell lung cancer (FLEX): an open-label randomised phase III trial. Lancet. 2009;373:1525–1531. - PubMed
-
- Van Cutsem E, Kohne CH, Hitre E, Zaluski J, Chien C. R. Chang, Makhson A, D’Haens G, Pinter T, Lim R, Bodoky G, Roh JK, Folprecht G, Ruff P, Stroh C, Tejpar S, Schlichting M, Nippgen J, Rougier P. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009;360:1408–1417. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
