

Developing risk prediction models for type 2 diabetes: a systematic review of methodology and reporting
- PMID: 21902820
- PMCID: PMC3180398
- DOI: 10.1186/1741-7015-9-103
Developing risk prediction models for type 2 diabetes: a systematic review of methodology and reporting
Abstract
Background: The World Health Organisation estimates that by 2030 there will be approximately 350 million people with type 2 diabetes. Associated with renal complications, heart disease, stroke and peripheral vascular disease, early identification of patients with undiagnosed type 2 diabetes or those at an increased risk of developing type 2 diabetes is an important challenge. We sought to systematically review and critically assess the conduct and reporting of methods used to develop risk prediction models for predicting the risk of having undiagnosed (prevalent) or future risk of developing (incident) type 2 diabetes in adults.
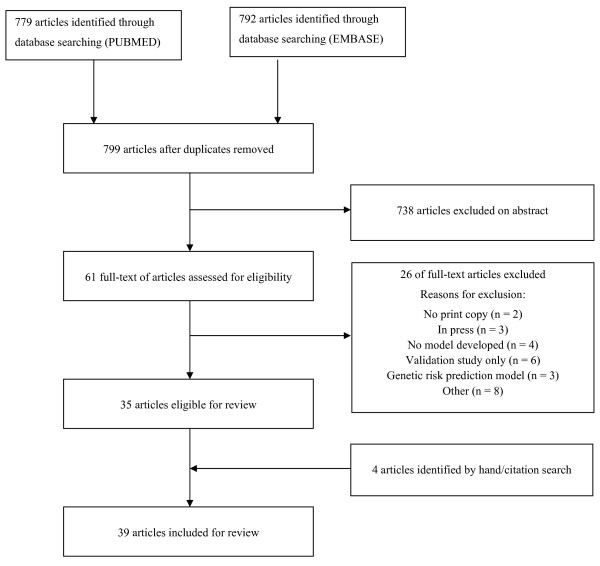
Methods: We conducted a systematic search of PubMed and EMBASE databases to identify studies published before May 2011 that describe the development of models combining two or more variables to predict the risk of prevalent or incident type 2 diabetes. We extracted key information that describes aspects of developing a prediction model including study design, sample size and number of events, outcome definition, risk predictor selection and coding, missing data, model-building strategies and aspects of performance.
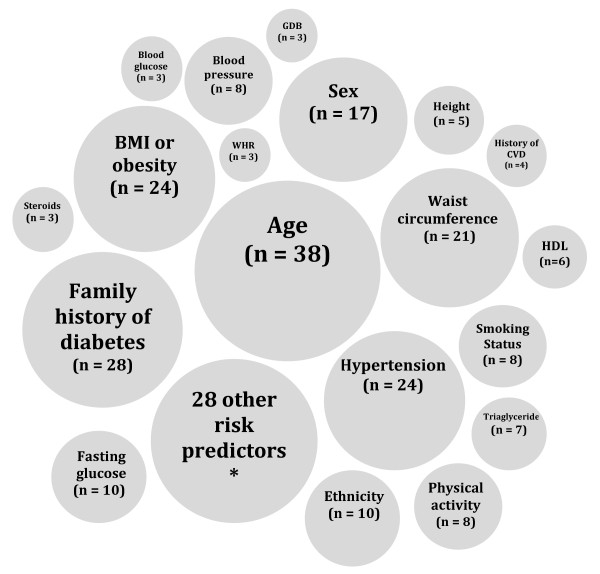
Results: Thirty-nine studies comprising 43 risk prediction models were included. Seventeen studies (44%) reported the development of models to predict incident type 2 diabetes, whilst 15 studies (38%) described the derivation of models to predict prevalent type 2 diabetes. In nine studies (23%), the number of events per variable was less than ten, whilst in fourteen studies there was insufficient information reported for this measure to be calculated. The number of candidate risk predictors ranged from four to sixty-four, and in seven studies it was unclear how many risk predictors were considered. A method, not recommended to select risk predictors for inclusion in the multivariate model, using statistical significance from univariate screening was carried out in eight studies (21%), whilst the selection procedure was unclear in ten studies (26%). Twenty-one risk prediction models (49%) were developed by categorising all continuous risk predictors. The treatment and handling of missing data were not reported in 16 studies (41%).
Conclusions: We found widespread use of poor methods that could jeopardise model development, including univariate pre-screening of variables, categorisation of continuous risk predictors and poor handling of missing data. The use of poor methods affects the reliability of the prediction model and ultimately compromises the accuracy of the probability estimates of having undiagnosed type 2 diabetes or the predicted risk of developing type 2 diabetes. In addition, many studies were characterised by a generally poor level of reporting, with many key details to objectively judge the usefulness of the models often omitted.
Figures
References
-
- Screening for Type 2 Diabetes: Report of a World Health Organization and International Diabetes Federation meeting. http://www.who.int/diabetes/publications/en/screening_mnc03.pdf
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
