

Age-related changes in aortic arch geometry: relationship with proximal aortic function and left ventricular mass and remodeling
- PMID: 21903061
- PMCID: PMC3508703
- DOI: 10.1016/j.jacc.2011.06.012
Age-related changes in aortic arch geometry: relationship with proximal aortic function and left ventricular mass and remodeling
Abstract
Objectives: We sought to define age-related geometric changes of the aortic arch and determine their relationship to central aortic stiffness and left ventricular (LV) remodeling.
Background: The proximal aorta has been shown to thicken, enlarge in diameter, and lengthen with aging in humans. However, no systematic study has described age-related longitudinal and transversal remodeling of the aortic arch and their relationship with LV mass and remodeling.
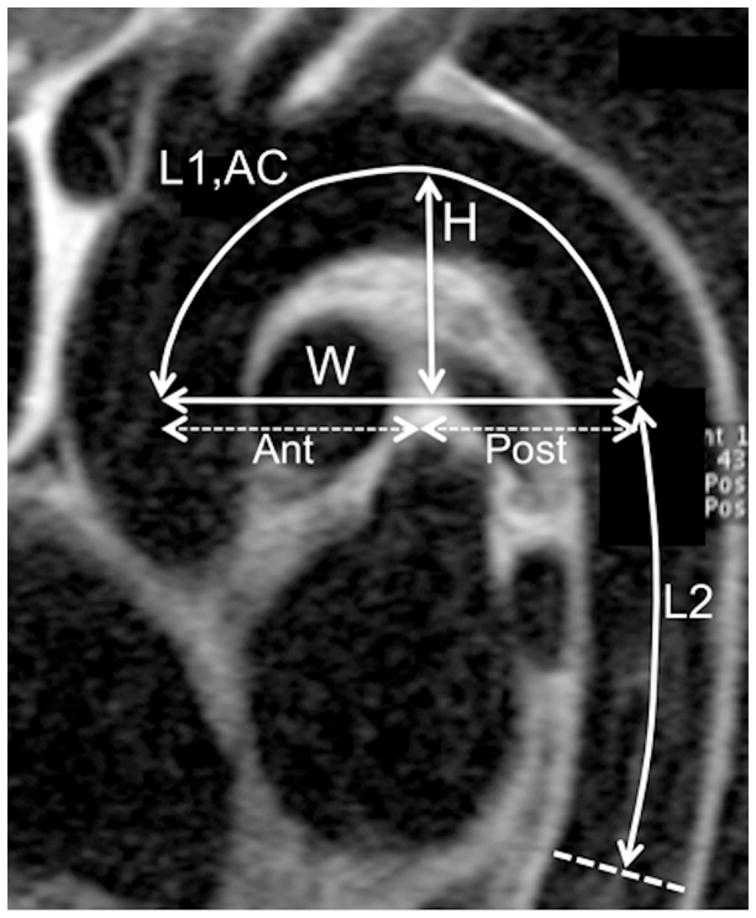
Methods: We studied 100 subjects (55 women, 45 men, average age 46 ± 16 years) free of overt cardiovascular disease using magnetic resonance imaging to determine aortic arch geometry (length, diameters, height, width, and curvature), aortic arch function (local aortic distensibility and arch pulse wave velocity [PWV]), and LV volumes and mass. Radial tonometry was used to calculate central blood pressure.
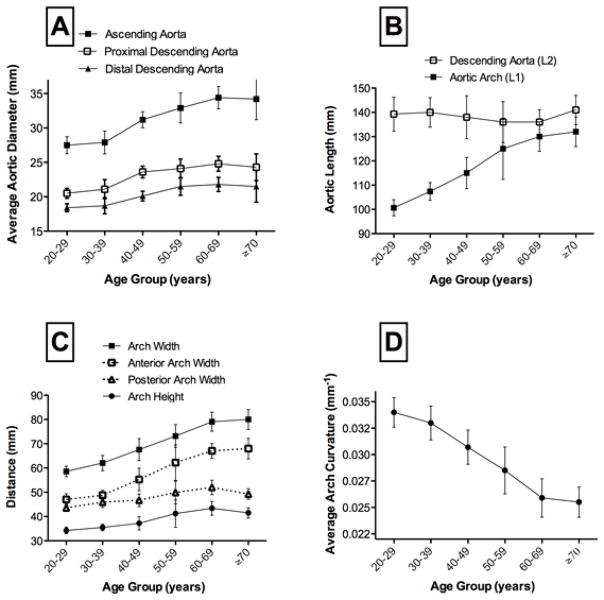
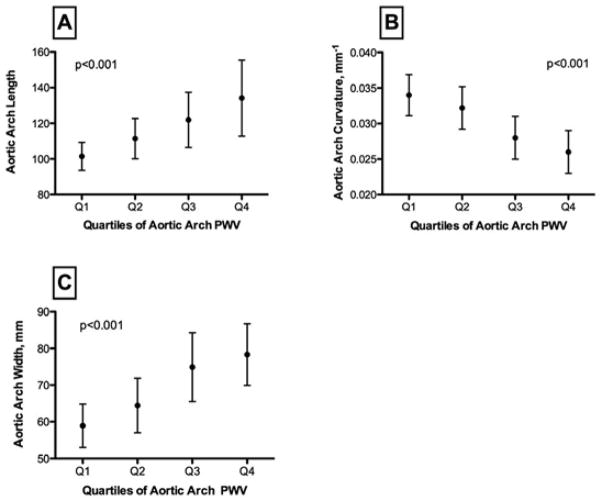
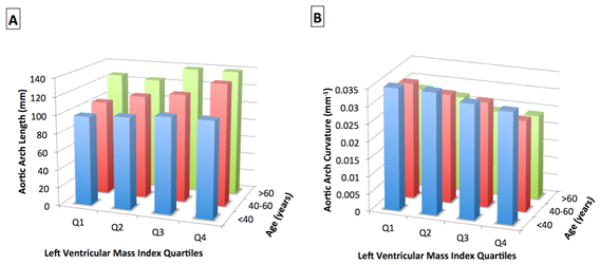
Results: Aortic diameters and arch length increased significantly with age. The ascending aorta length increased most, with age leading to aortic arch widening and decreased curvature. These geometric changes of the aortic arch were significantly related to decreased ascending aortic distensibility, increased aortic arch PWV (p < 0.001), and increased central blood pressures (p < 0.001). Increased ascending aortic diameter, lengthening, and decreased curvature of the aortic arch (unfolding) were all significantly associated with increased LV mass and concentric remodeling independently of age, sex, body size, and central blood pressure (p < 0.01).
Conclusions: Age-related unfolding of the aortic arch is related to increased proximal aortic stiffness in individuals without cardiovascular disease and associated with increased LV mass and mass-to-volume ratio independent of age, body size, central pressure, and cardiovascular risk factors.
Copyright © 2011 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Lakatta EG, Levy D. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: Part I: aging arteries: a « set up » for vascular disease. Circulation. 2003;107 (1):139–46. - PubMed
-
- O’Rourke MF, Staessen JA, Vlachopoulos C, Duprez D, Plante GE. Clinical applications of arterial stiffness; definitions and reference values. Am J Hypertens. 2002;15 (5):426–444. - PubMed
-
- Laurent S, Cockcroft J, Van Bortel L, et al. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27 (21):2588–2605. - PubMed
-
- Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of Cardiovascular Events and All-Cause Mortality With Arterial Stiffness: A Systematic Review and Meta-Analysis. J Am Coll Cardiol. 2010;55 (13):1318–1327. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
