

Computer simulation of nerve transfer strategies for restoring shoulder function after adult C5 and C6 root avulsion injuries
- PMID: 21903345
- PMCID: PMC3197221
- DOI: 10.1016/j.jhsa.2011.07.019
Computer simulation of nerve transfer strategies for restoring shoulder function after adult C5 and C6 root avulsion injuries
Abstract
Purpose: Functional ability after nerve transfer for upper brachial plexus injuries relies on both the function and magnitude of force recovery of targeted muscles. Following nerve transfers targeting either the axillary nerve, suprascapular nerve, or both, it is unclear whether functional ability is restored in the face of limited muscle force recovery.
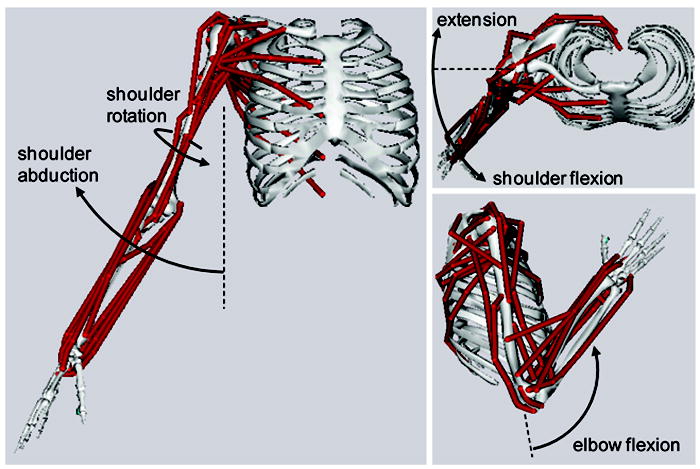
Methods: We used a computer model to simulate flexing the elbow while maintaining a functional shoulder posture for 3 nerve transfer scenarios. We assessed the minimum restored force capacity necessary to perform the task, the associated compensations by neighboring muscles, and the effect of altered muscle coordination on movement effort.
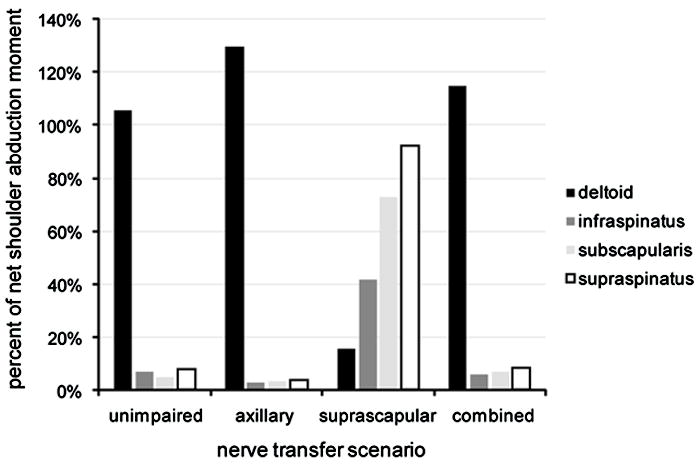
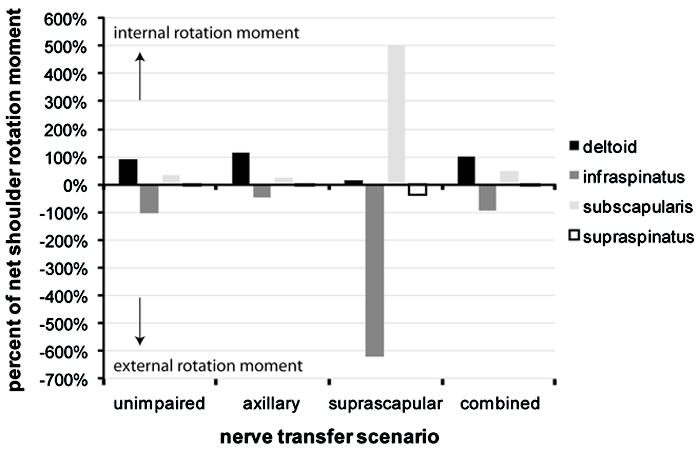
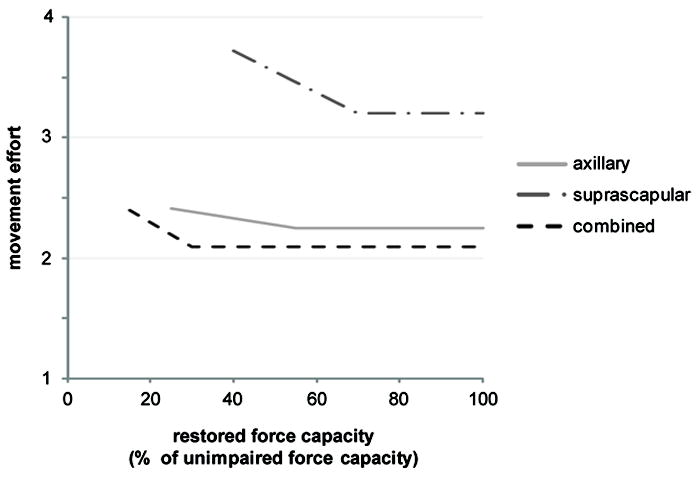
Results: The minimum force restored by the axillary, suprascapular, and combined nerve transfers that was required for the model to simulate the desired movement was 25%, 40%, and 15% of the unimpaired muscle force capacity, respectively. When the deltoid was paralyzed, the infraspinatus and subscapularis muscles generated higher shoulder abduction moments to compensate for deltoid weakness. For all scenarios, movement effort increased as restored force capacity decreased.
Conclusions: Combined axillary and suprascapular nerve transfer required the least restored force capacity to perform the desired elbow flexion task, whereas single suprascapular nerve transfer required the most restored force capacity to perform the same task. Although compensation mechanisms allowed all scenarios to perform the desired movement despite weakened shoulder muscles, compensation increased movement effort. Dynamic simulations allowed independent evaluation of the effect of restored force capacity on functional outcome in a way that is not possible experimentally.
Clinical relevance: Simultaneous nerve transfer to suprascapular and axillary nerves yields the best simulated biomechanical outcome for lower magnitudes of muscle force recovery in this computer model. Axillary nerve transfer performs nearly as well as the combined transfer, whereas suprascapular nerve transfer is more sensitive to the magnitude of reinnervation and is therefore avoided.
Copyright © 2011 American Society for Surgery of the Hand. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Rankine JJ. Adult traumatic brachial plexus injury. Clin Radiol. 2004;59:767–774. - PubMed
-
- Bertelli JA, Ghizoni MF. Reconstruction of C5 and C6 Brachial Plexus Avulsion Injury by Multiple Nerve Transfers: Spinal Accessory to Suprascapular, Ulnar Fascicles to Biceps Branch, and Triceps Long or Lateral Head Branch to Axillary Nerve. J Hand Surg. 2004;29A:131–139. - PubMed
-
- Merrell GA, Barrie KA, Katz DL, Wolfe SW. Results of nerve transfer techniques for restoration of shoulder and elbow function in the context of a meta-analysis of the English literature. J Hand Surg. 2001;26:303–314. - PubMed
-
- Terzis JK, Kostas I. Suprascapular Nerve Reconstruction in 118 Cases of Adult Posttraumatic Brachial Plexus. Plastic & Reconstr Surg. 2006;117:613–629. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
