

FGF-23 associates with death, cardiovascular events, and initiation of chronic dialysis
- PMID: 21903574
- PMCID: PMC3187186
- DOI: 10.1681/ASN.2010121224
FGF-23 associates with death, cardiovascular events, and initiation of chronic dialysis
Abstract
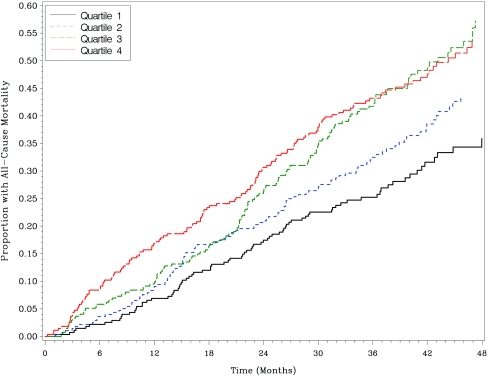
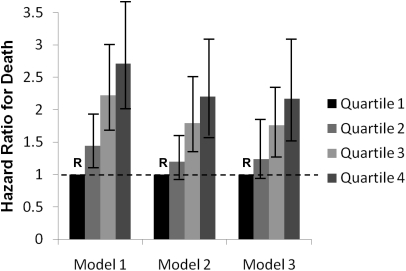
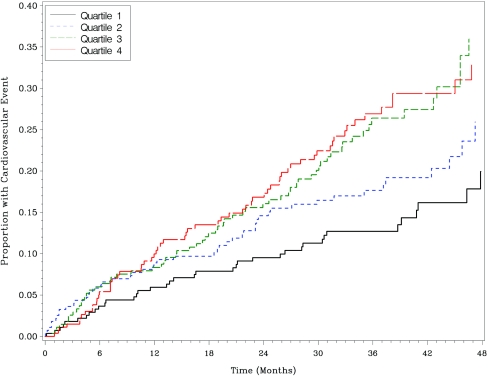
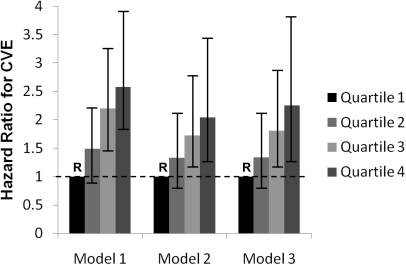
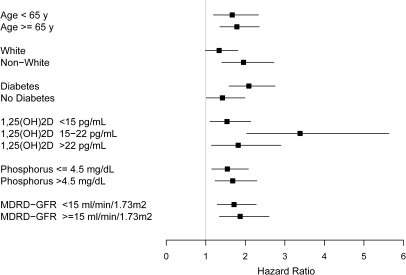
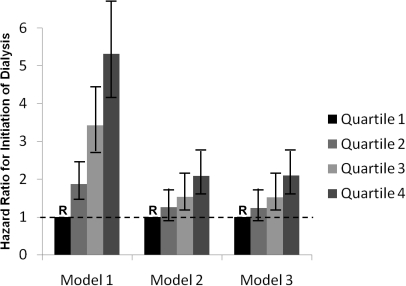
Concentrations of the phosphate-regulating hormone fibroblast growth factor-23 (FGF-23) are elevated in patients with chronic kidney disease (CKD), but whether higher plasma FGF-23 concentrations associate with all-cause mortality, cardiovascular events, or initiation of chronic dialysis is not completely understood. Here, we measured FGF-23 concentration in stored plasma samples from 1099 patients with advanced CKD who participated in The Homocysteine in Kidney and End Stage Renal Disease study. Mean serum phosphorus concentration was 4.3 mg/dl, median FGF-23 concentration was 392 RU/ml, and mean GFR was 18 ml/min/1.73 m(2). During a median follow-up of 2.9 yr, 453 (41%) patients died from any cause, 215 (20%) had a cardiovascular event, and 615 (56%) initiated chronic dialysis. Compared with the lowest quartile of FGF-23, each subsequent quartile associated with a progressively higher risk for death, adjusted for confounders (HR [95% CI] of 1.24 [0.91 to 1.69], 1.76 [1.28 to 2.44], and 2.17 [1.56 to 3.08] for the second through fourth quartiles, respectively). In addition, compared with the lowest quartile, the two highest quartiles of FGF-23 also associated with a significantly elevated risk for cardiovascular events and initiation of chronic dialysis. In conclusion, in advanced CKD, FGF-23 strongly and independently associates with all-cause mortality, cardiovascular events, and initiation of chronic dialysis.
Figures
Comment in
-
Risk factors: Levels of FGF23 predict outcomes in advanced CKD.Nat Rev Nephrol. 2011 Oct 4;7(11):606. doi: 10.1038/nrneph.2011.130. Nat Rev Nephrol. 2011. PMID: 21971190 No abstract available.
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van Lente F, Levey AS: Prevalence of chronic kidney disease in the United States. JAMA 298: 2038–2047, 2007 - PubMed
-
- Keith DS, Nichols GA, Gullion CM, Brown JB, Smith DH: Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Intern Med 164: 659–663, 2004 - PubMed
-
- Shlipak MG, Fried LF, Cushman M, Manolio TA, Peterson D, Stehman-Breen C, Bleyer A, Newman A, Siscovick D, Psaty B: Cardiovascular mortality risk in chronic kidney disease: Comparison of traditional and novel risk factors. JAMA 293: 1737–1745, 2005 - PubMed
-
- Hage FG, Venkataraman R, Zoghbi GJ, Perry GJ, DeMattos AM, Iskandrian AE: The scope of coronary heart disease in patients with chronic kidney disease. J Am Coll Cardiol 53: 2129–2140, 2009 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
