

Cardiac magnetic resonance assessment of left ventricular mass in autosomal dominant polycystic kidney disease
- PMID: 21903983
- PMCID: PMC3186455
- DOI: 10.2215/CJN.04610511
Cardiac magnetic resonance assessment of left ventricular mass in autosomal dominant polycystic kidney disease
Abstract
Background and objectives: Autosomal dominant polycystic kidney disease (ADPKD) is associated with a substantial cardiovascular disease burden including early onset hypertension, intracranial aneurysms, and left ventricular hypertrophy (LVH). A 41% prevalence of LVH has been reported in ADPKD, using echocardiographic assessment of LV mass (LVM). The HALT PKD study was designed to assess the effect of intensive angiotensin blockade on progression of total kidney volume and LVM. Measurements of LVM were performed using cardiac magnetic resonance (MR).
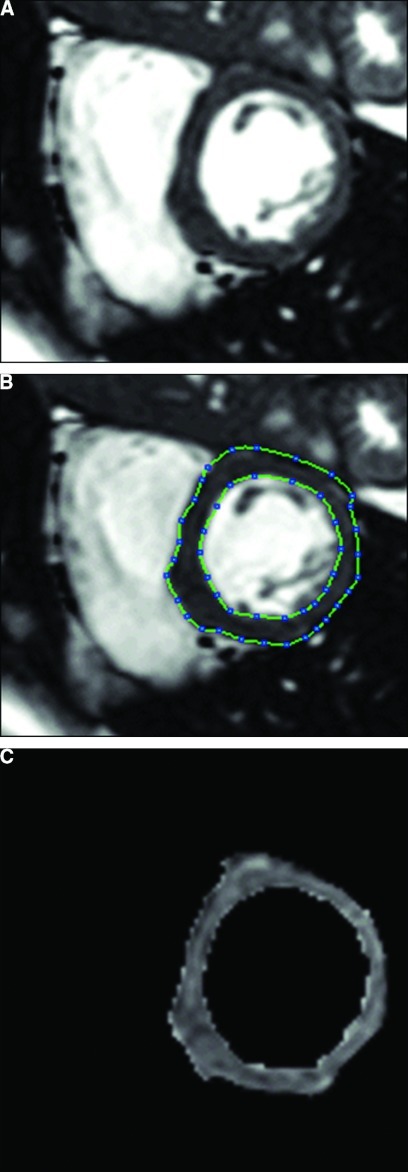
Design, setting, participants, & measurements: Five hundred forty-three hypertensive patients with GFR >60 ml/min per 1.73 m(2) underwent MR assessment of LVM at baseline. LVM was adjusted for body surface area and expressed as LVM index (LVMI; g/m(2)).
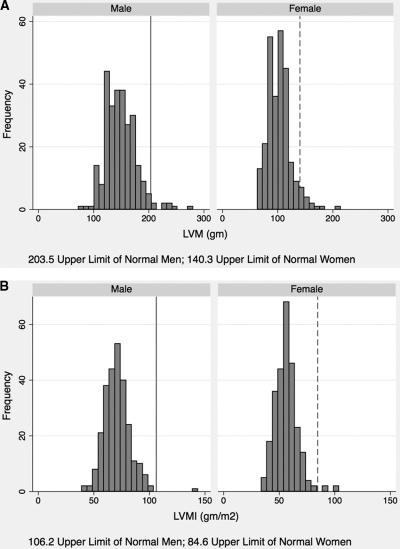
Results: Baseline BP was 125.1 ± 14.5/79.3 ± 11.6 mmHg. Average duration of hypertension was 5.79 years. Prior use of angiotensin-converting enzyme inhibitors or angiotensin receptor blockers was present in 59.5% of patients. The prevalence of LVH assessed using nonindexed LVM (g) was 3.9% (n = 21, eight men and 13 women) and 0.93% (n = 5, one man and four women) using LVMI (g/m(2)). In exploratory analyses, the prevalence of LVH using LVM indexed to H(2.7), and the allometric index ppLVmass(HW), ranged from 0.74% to 2.23% (n = 4 to 12). Multivariate regression showed significant direct associations of LVMI with systolic BP, serum creatinine, and albuminuria; significant inverse associations with LVMI were found with age and female gender.
Conclusions: The prevalence of LVH in hypertensive ADPKD patients <50 years of age with short duration of hypertension, and prior use of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers is low. Early BP intervention in ADPKD may have decreased LVH and may potentially decrease cardiovascular mortality.
Figures
References
-
- Hateboer N, v Dijk M, Bogdanova N, Coto E, Saggar-Malik A, San Millan J, Torra R, Breuning M, Ravine D: Comparison of phenotypes of polycystic kidney disease types 1 and 2. European PKD1-PKD2 Study Group Lancet 353(9147): 103–107, 1999 - PubMed
-
- Schrier R: Renal volume, renin-angiotensin-aldosterone system, hypertension, and left ventricular hypertrophy in patients with autosomal dominant polycystic kidney disease. J Am Soc Nephrol 20: 1888–1893, 2009 - PubMed
-
- Perrone R, Ruthazer R, Terrin N: Survival after end-stage renal disease in autosomal dominant polycystic kidney disease: Contribution of extrarenal complications to mortality. Am J Kidney Dis 38: 777–784, 2001 - PubMed
-
- Fick G, Johnson A, Hammond W, Gabow P: Causes of death in autosomal dominant polycystic kidney disease. J Am Soc Nephrol 5: 2048–2056, 1995 - PubMed
-
- Ivy D, Shaffer E, Johnson A, Kimberling W, Dobin A, Gabow P: Cardiovascular abnormalities in children with autosomal dominant polycystic kidney disease. J Am Soc Nephrol 5: 2032–2036, 1995 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- M01 RR000585/RR/NCRR NIH HHS/United States
- U01 DK062402/DK/NIDDK NIH HHS/United States
- DK62410/DK/NIDDK NIH HHS/United States
- UL1 RR025752/RR/NCRR NIH HHS/United States
- M01 RR000039/RR/NCRR NIH HHS/United States
- UL1 RR024992/RR/NCRR NIH HHS/United States
- DK62402/DK/NIDDK NIH HHS/United States
- DK62408/DK/NIDDK NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- M01 RR000051/RR/NCRR NIH HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
- U01 DK062411/DK/NIDDK NIH HHS/United States
- UL1 RR025008/RR/NCRR NIH HHS/United States
- RR23940/RR/NCRR NIH HHS/United States
- RR000051/RR/NCRR NIH HHS/United States
- RR00585/RR/NCRR NIH HHS/United States
- U01 DK062401/DK/NIDDK NIH HHS/United States
- DK62401/DK/NIDDK NIH HHS/United States
- UL1 RR025780/RR/NCRR NIH HHS/United States
- M01 RR000054/RR/NCRR NIH HHS/United States
- M01 RR023940/RR/NCRR NIH HHS/United States
- RR000054/RR/NCRR NIH HHS/United States
- U01 DK062408/DK/NIDDK NIH HHS/United States
- U01 DK082230/DK/NIDDK NIH HHS/United States
- UL1 RR024150/RR/NCRR NIH HHS/United States
- RR000039/RR/NCRR NIH HHS/United States
- DK62411/DK/NIDDK NIH HHS/United States
- U01 DK062410/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
