

Lack of consistent intracranial pressure pulse morphological changes during episodes of microdialysis lactate/pyruvate ratio increase
- PMID: 21904021
- PMCID: PMC3334323
- DOI: 10.1088/0967-3334/32/10/011
Lack of consistent intracranial pressure pulse morphological changes during episodes of microdialysis lactate/pyruvate ratio increase
Abstract
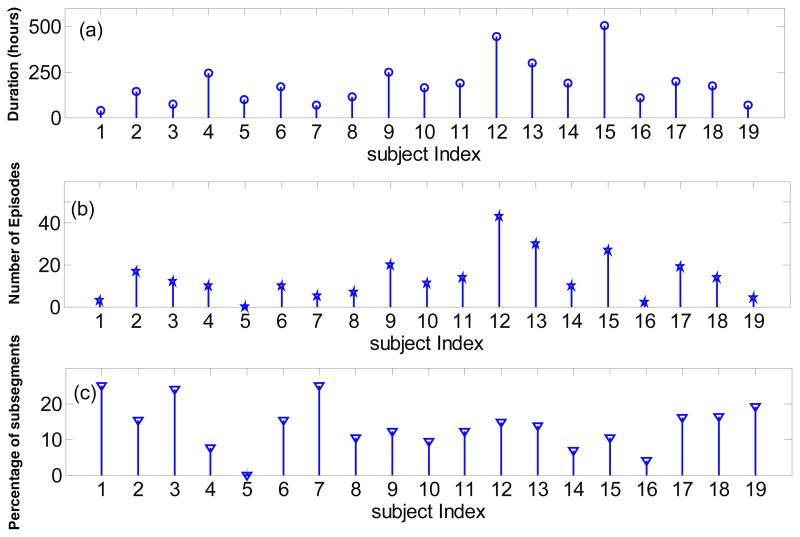
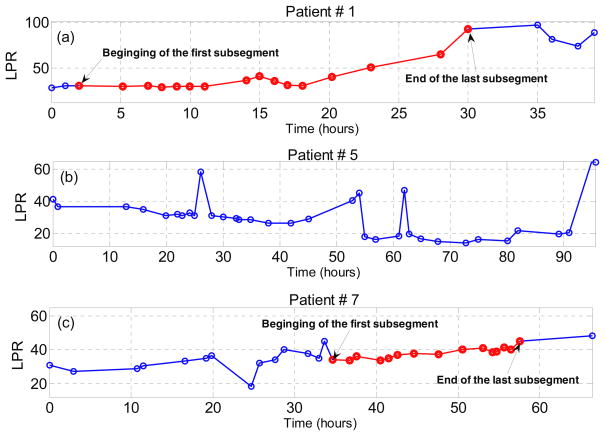
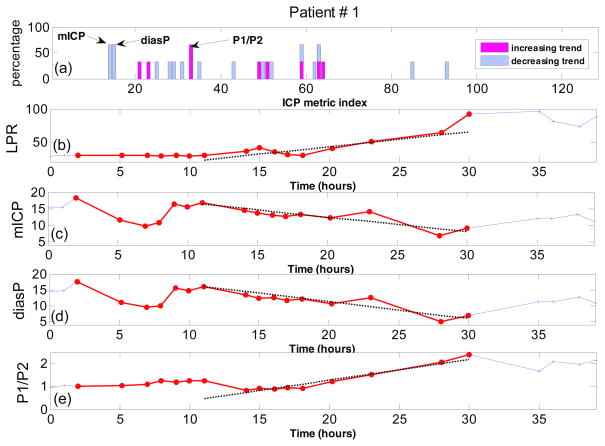
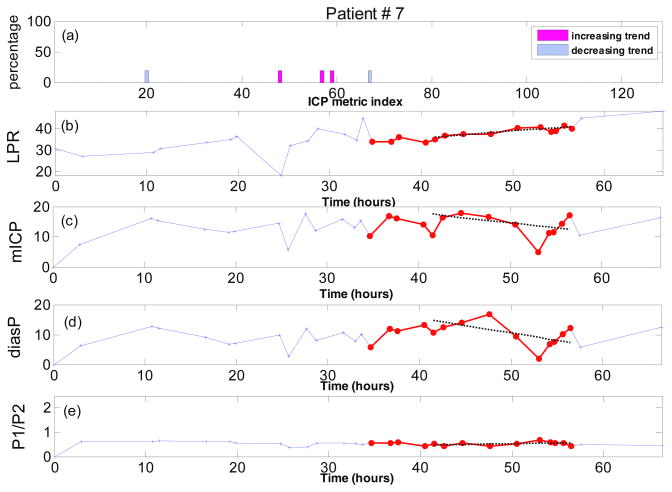
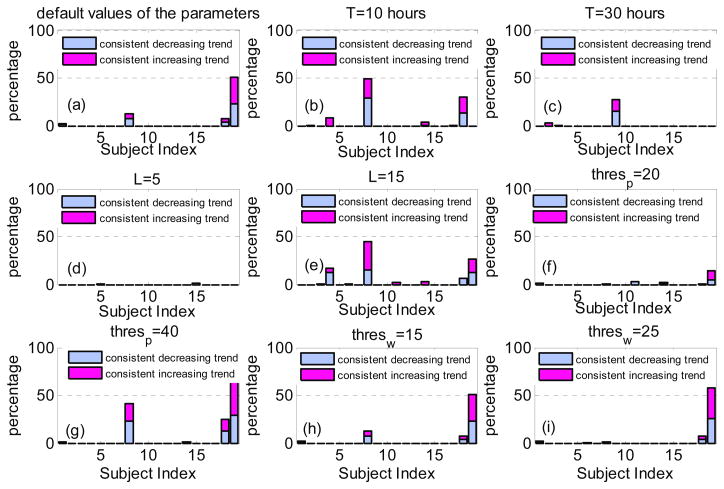
Lactate/pyruvate ratio (LPR) from microdialysis is a well-established marker of cerebral metabolic crisis. For brain injury patients, abnormally high LPR could indicate cerebral ischemia or failure of O(2) uptake. However, there is a debate on the primary factor responsible for LPR increase. Exploiting the potential of using the morphology of a high temporal resolution signal such as intracranial pulse (ICP) to characterize cerebrovascular changes, a data analysis experiment is taken to test whether consistent changes in ICP pulse morphological metrics accompany the LPR increase. We studied 3517 h of LPR and continuous ICP data from 19 severe traumatic brain injury patients. Our morphological clustering and analysis of intracranial pressure (MOCAIP) algorithm was applied to ICP pulses, which were matched in time to the LPR measurements, and 128 pulse morphological metrics were extracted. We automatically identified the episodes of LPR increases using a moving time window of 10-20 h. We then studied the trending patterns of each of the 128 ICP MOCAIP metrics within these identified periods and determined them to be one of the following three types: increasing, decreasing or no trend. A binomial test was employed to investigate whether any MOCAIP metrics show a consistent trend among all episodes of LPR increase per patient. Regardless of the selected values for different parameters of the proposed method, for the majority of the subjects in the study (78%), none of the ICP metrics show any consistent trend during the episodes of LPR increase. Even for the few subjects who have at least one ICP metric with a consistent trend during the LPR increase episodes, the number of such metrics is small and varies from subject to subject. Given the fact that ICP pulse morphology is influenced by the cerebral vasculature, our results suggest that a dominant cerebral vascular cause may be behind the changes in LPR when LPR trends correlate with ICP pulse morphological changes. However, the incidence of such correlation seems to be low.
Figures
References
-
- Adolph RJ, Fukusumi H, Fowler NO. Origin of cerebrospinal fluid pulsations. The American journal of physiology. 1967;212:840–6. - PubMed
-
- Bjerring PN, Hauerberg J, Jorgensen L, Frederiksen HJ, Tofteng F, Hansen BA, Larsen FS. Brain hypoxanthine concentration correlates to lactate/pyruvate ratio but not intracranial pressure in patients with acute liver failure. Journal of hepatology. 2010;53:1054–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources