

An update on the use of gonadotropin-releasing hormone antagonists in prostate cancer
- PMID: 21904569
- PMCID: PMC3159401
- DOI: 10.1177/1756287211414457
An update on the use of gonadotropin-releasing hormone antagonists in prostate cancer
Abstract
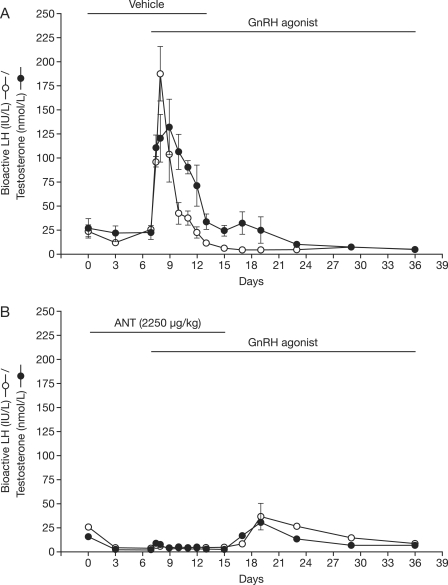
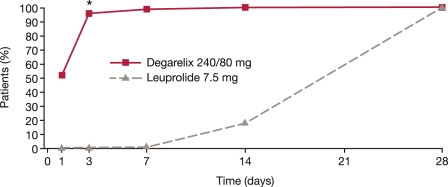
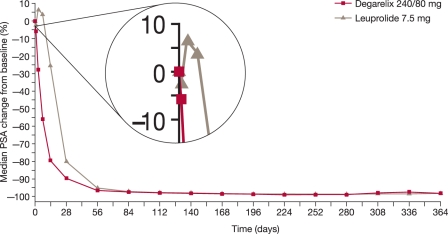
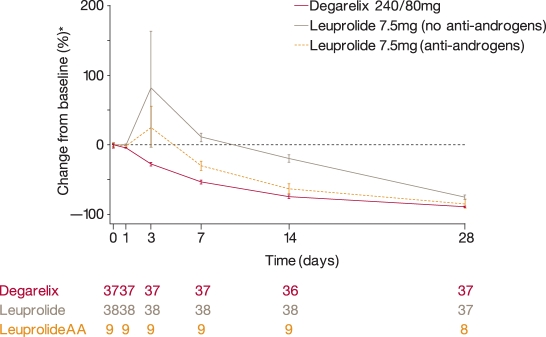
Androgen deprivation therapy (ADT) is the main treatment approach in advanced prostate cancer and in recent years has primarily involved the use of gonadotropin-releasing hormone (GnRH) agonists. However, despite their efficacy, GnRH agonists have several drawbacks associated with their mode of action. These include an initial testosterone surge and testosterone microsurges on repeat administration. GnRH antagonists provide an alternative approach to ADT with a more direct mode of action that involves immediate blockade of GnRH receptors. Antagonists produce a more rapid suppression of testosterone (and prostate-specific antigen [PSA]) without a testosterone surge or microsurges and appear to offer an effective and well tolerated option for the hormonal treatment of prostate cancer. Comparisons with GnRH agonists have shown GnRH antagonists to be at least as effective in achieving and maintaining castrate testosterone levels in patients with prostate cancer. Furthermore, with antagonists, the lack of an initial testosterone surge (which may cause clinical flare) may allow more rapid relief of symptoms related to prostate cancer, avoid the need for concomitant antiandrogens to prevent clinical flare (so avoiding any antiandrogen-associated adverse events) and allow GnRH antagonist use in patients with high tumour burden and/or acute problems such as spinal cord compression. Although several antagonists have been investigated, only degarelix and abarelix are currently available for clinical use in prostate cancer. Currently, degarelix is the most extensively studied and widely available agent in this class. Degarelix is one of a newer generation of antagonists which, in a comprehensive and ongoing clinical development programme, has been shown to provide rapid, profound and sustained testosterone suppression without the systemic allergic reactions associated with earlier antagonists. This review examines the currently available data on GnRH antagonists in prostate cancer.
Keywords: GnRH agonist; GnRH antagonist; abarelix; degarelix; prostate cancer.
Figures
References
-
- Amory J.K., Leonard T.W., Page S.T., O'Toole E., McKenna M.J., Bremner W.J. (2009) Oral administration of the GnRH antagonist acyline, in a GIPET-enhanced tablet form, acutely suppresses serum testosterone in normal men: single-dose pharmacokinetics and pharmacodynamics. Cancer Chemother Pharmacol 64: 641–645 - PMC - PubMed
-
- Boccon-Gibod L., Klotz L., Schröder H., Andreou C., Persson B.E., Cantor P., et al. (2008) Degarelix compared to leuprolide depot 7.5 mg in a 12-month randomised, open-label, parallel-group phase III study in prostate cancer patients. Eur Urol (Suppl. 7): 205–205 abstract 537
-
- Broqua P., Riviere P.J., Conn P.M., Rivier J.E., Aubert M.L., Junien J.L. (2002) Pharmacological profile of a new, potent, and longacting gonadotropin-releasing hormone antagonist: degarelix. J Pharmacol Exp Ther 301: 95–102 - PubMed
-
- Castellón E., Clementi M., Hitschfeld C., Sánchez C., Benítez D., Sáenz L., et al. (2006) Effect of leuprolide and cetrorelix on cell growth, apoptosis, and GnRH receptor expression in primary cell cultures from human prostate carcinoma. Cancer Invest 24: 261–268 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
