

A framework for quantifying net benefits of alternative prognostic models
- PMID: 21905066
- PMCID: PMC3496857
- DOI: 10.1002/sim.4362
A framework for quantifying net benefits of alternative prognostic models
Abstract
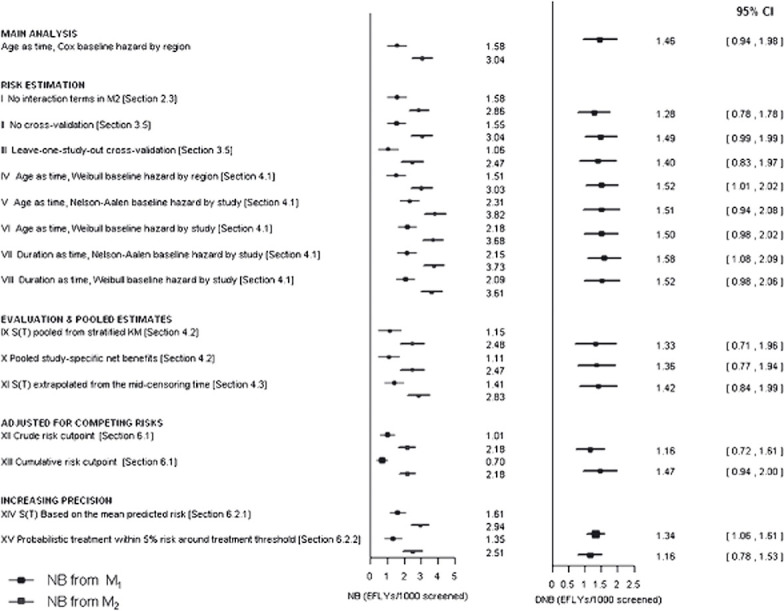
New prognostic models are traditionally evaluated using measures of discrimination and risk reclassification, but these do not take full account of the clinical and health economic context. We propose a framework for comparing prognostic models by quantifying the public health impact (net benefit) of the treatment decisions they support, assuming a set of predetermined clinical treatment guidelines. The change in net benefit is more clinically interpretable than changes in traditional measures and can be used in full health economic evaluations of prognostic models used for screening and allocating risk reduction interventions. We extend previous work in this area by quantifying net benefits in life years, thus linking prognostic performance to health economic measures; by taking full account of the occurrence of events over time; and by considering estimation and cross-validation in a multiple-study setting. The method is illustrated in the context of cardiovascular disease risk prediction using an individual participant data meta-analysis. We estimate the number of cardiovascular-disease-free life years gained when statin treatment is allocated based on a risk prediction model with five established risk factors instead of a model with just age, gender and region. We explore methodological issues associated with the multistudy design and show that cost-effectiveness comparisons based on the proposed methodology are robust against a range of modelling assumptions, including adjusting for competing risks.
Copyright © 2011 John Wiley & Sons, Ltd.
Figures
References
-
- Pyorala K, De Backer G, Graham I, et al. Prevention of coronary heart disease in clinical practice. Recommendations of the Task Force of the European Society of Cardiology, European Atherosclerosis Society and European Society of Hypertension. European Heart Journal. 1994;15:1300–31. - PubMed
-
- Harrell FE, Lee KL, Mark DB. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Statistics in Medicine. 1996;15:361–387. DOI: 10.1002/(SICI)1097-0258(19960229)15:4<361::AID-SIM168>3.0.CO;2-4. - DOI - PubMed
-
- Cook NR. Use and misuse of the receiver operating characteristic curve in risk prediction. Circulation. 2007;115:928–935. DOI: 10.1161/CIRCULATIONAHA.106.672402. - DOI - PubMed
-
- Ridker PM, Buring JE, Rifai N, Cook NR. Development and validation of improved algorithms for the assessment of global cardiovascular risk in women: The Reynolds risk score. Journal of the American Medical Association. 2007;297:611–9. DOI: 10.1001/jama.297.12.1376. - DOI - PubMed
-
- Pencina MJ, D'Agostino Sr RB, D'Agostino Jr RB, Vasan RS. Evaluating the added predictive ability of a new marker: From area under the ROC curve to reclassification and beyond. Statistics in Medicine. 2008;27:157–172. DOI: 10.1002/sim.2929. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
- G19/35/MRC_/Medical Research Council/United Kingdom
- G0700463/MRC_/Medical Research Council/United Kingdom
- G0100222/MRC_/Medical Research Council/United Kingdom
- U.1052.00.006/MRC_/Medical Research Council/United Kingdom
- UL1 TR000062/TR/NCATS NIH HHS/United States
- G0701619/MRC_/Medical Research Council/United Kingdom
- RG/08/014/24067/BHF_/British Heart Foundation/United Kingdom
- MC_U105260792/MRC_/Medical Research Council/United Kingdom
- G8802774/MRC_/Medical Research Council/United Kingdom
- RG/08/013/25942/BHF_/British Heart Foundation/United Kingdom
- G0902037/MRC_/Medical Research Council/United Kingdom
- U.1052.00.001/MRC_/Medical Research Council/United Kingdom
- MC_U105260558/MRC_/Medical Research Council/United Kingdom
- RG/07/008/23674/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
