

Impact of donor left ventricular hypertrophy on survival after heart transplant
- PMID: 21906259
- PMCID: PMC3602908
- DOI: 10.1111/j.1600-6143.2011.03744.x
Impact of donor left ventricular hypertrophy on survival after heart transplant
Abstract
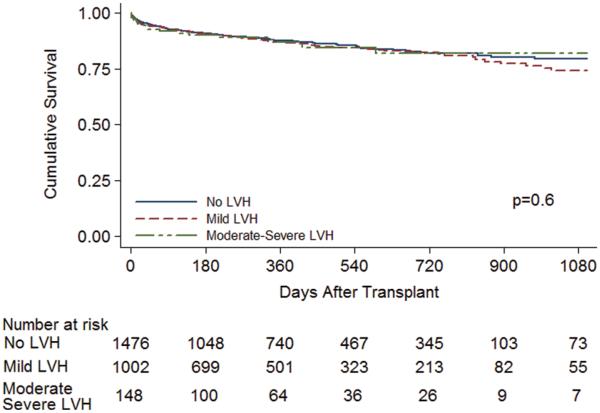
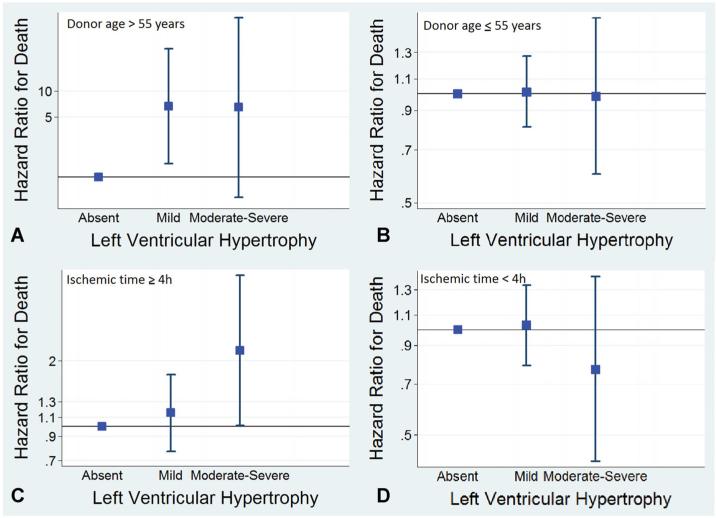
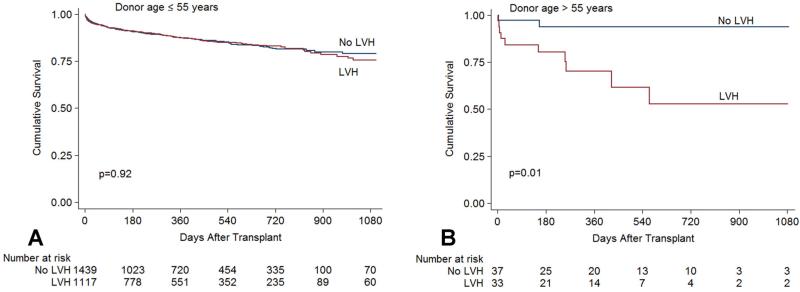
Left ventricular hypertrophy (LVH) of the donor heart is believed to increase the risk of allograft failure after transplant. However this effect is not well quantified, with variable findings from single-center studies. The United Network for Organ Sharing database was used to analyze the effect of donor LVH on recipient survival. Three cohorts, selected in accordance with the American Society of Echocardiography guidelines, were examined: recipients of allografts without LVH (<1.1 cm), with mild LVH (1.1-1.3 cm) and with moderate-severe LVH (≥ 1.4 cm). The study group included 2626 patients with follow-up of up to 3.3 years. Mild LVH was present in 38% and moderate-severe LVH in 5.6% of allografts. Predictors of mortality included a number of donor and recipient characteristics, but not LVH. However, a subgroup analysis showed an increased risk of death in recipients of allografts with LVH and donor age >55 years, and in recipients of allografts with LVH and ischemic time ≥ 4 h. In the contemporary era, close to half of all transplanted allografts demonstrate LVH, and survival of these recipients is similar to those without LVH. However, the use of allografts with LVH in association with other high-risk characteristics may result in increased mortality.
©Copyright 2011 The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures

References
-
- Stehlik J, Edwards LB, Kucheryavaya AY, et al. The registry of the international society for heart and lung transplantation: Twenty-seventh official adult heart transplant report—2010. J Heart Lung Transplant. 2010;29:1089–1103. - PubMed
-
- Copeland JG, Emery RW, Levinson MM, et al. Selection of patients for cardiac transplantation. Circulation. 1987;75:2–9. - PubMed
-
- Sweeney MS, Lammermeier DE, Frazier OH, Burnett CM, Haupt HM, Duncan JM. Extension of donor criteria in cardiac transplantation: Surgical risk versus supply-side economics. Ann Thorac Surg. 1990;50:7–10. - PubMed
-
- Jeevanandam V, Furukawa S, Prendergast TW, Todd BA, Eisen HJ, McClurken JB. Standard criteria for an acceptable donor heart are restricting heart transplantation. Ann Thorac Surg. 1996;62:1268–1275. - PubMed
-
- Zaroff JG, Rosengard BR, Armstrong WF, et al. Consensus conference report: Maximizing use of organs recovered from the cadaver donor: Cardiac recommendations, March 28-29, 2001, Crystal City, Va. Circulation. 2002;106:836–841. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
