

Technology assessment of automated atlas based segmentation in prostate bed contouring
- PMID: 21906279
- PMCID: PMC3180272
- DOI: 10.1186/1748-717X-6-110
Technology assessment of automated atlas based segmentation in prostate bed contouring
Abstract
Background: Prostate bed (PB) contouring is time consuming and associated with inter-observer variability. We evaluated an automated atlas-based segmentation (AABS) engine in its potential to reduce contouring time and inter-observer variability.
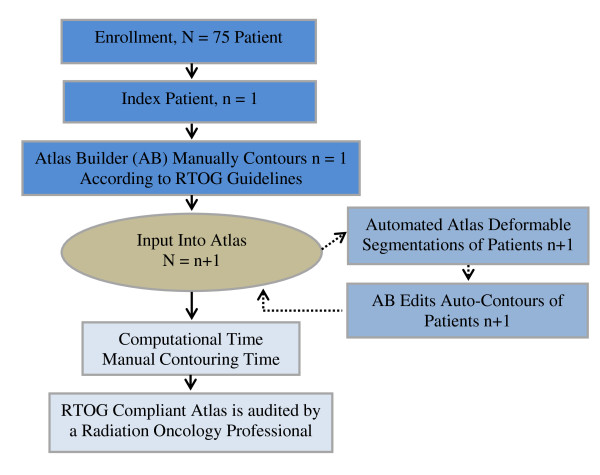
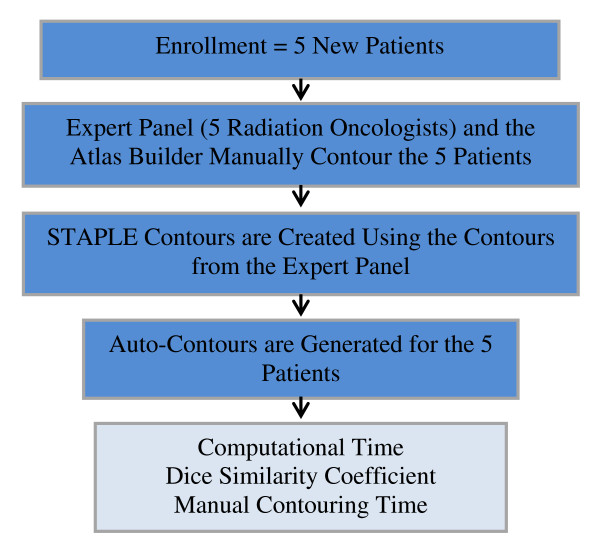
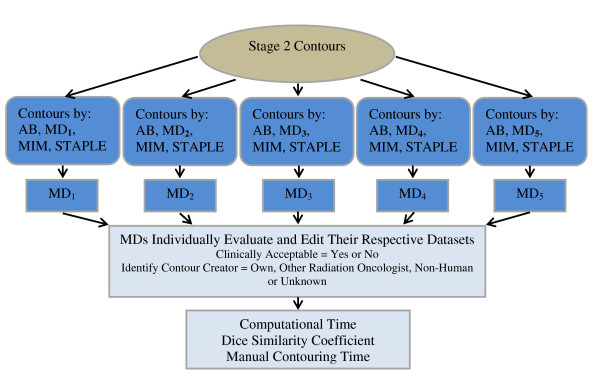
Methods: An atlas builder (AB) manually contoured the prostate bed, rectum, left femoral head (LFH), right femoral head (RFH), bladder, and penile bulb of 75 post-prostatectomy cases to create an atlas according to the recent RTOG guidelines. 5 other Radiation Oncologists (RO) and the AABS contoured 5 new cases. A STAPLE contour for each of the 5 patients was generated. All contours were anonymized and sent back to the 5 RO to be edited as clinically necessary. All contouring times were recorded. The dice similarity coefficient (DSC) was used to evaluate the unedited- and edited- AABS and inter-observer variability among the RO. Descriptive statistics, paired t-tests and a Pearson correlation were performed. ANOVA analysis using logit transformations of DSC values was calculated to assess inter-observer variability.
Results: The mean time for manual contours and AABS was 17.5- and 14.1 minutes respectively (p = 0.003). The DSC results (mean, SD) for the comparison of the unedited-AABS versus STAPLE contours for the PB (0.48, 0.17), bladder (0.67, 0.19), LFH (0.92, 0.01), RFH (0.92, 0.01), penile bulb (0.33, 0.25) and rectum (0.59, 0.11). The DSC results (mean, SD) for the comparison of the edited-AABS versus STAPLE contours for the PB (0.67, 0.19), bladder (0.88, 0.13), LFH (0.93, 0.01), RFH (0.92, 0.01), penile bulb (0.54, 0.21) and rectum (0.78, 0.12). The DSC results (mean, SD) for the comparison of the edited-AABS versus the expert panel for the PB (0.47, 0.16), bladder (0.67, 0.18), LFH (0.83, 0.18), RFH (0.83, 0.17), penile bulb (0.31, 0.23) and rectum (0.58, 0.09). The DSC results (mean, SD) for the comparison of the STAPLE contours and the 5 RO are PB (0.78, 0.15), bladder (0.96, 0.02), left femoral head (0.87, 0.19), right femoral head (0.87, 0.19), penile bulb (0.70, 0.17) and the rectum (0.89, 0.06). The ANOVA analysis suggests inter-observer variability among at least one of the 5 RO (p value = 0.002).
Conclusion: The AABS tool results in a time savings, and when used to generate auto-contours for the femoral heads, bladder and rectum had superior to good spatial overlap. However, the generated auto-contours for the prostate bed and penile bulb need improvement.
Figures
Similar articles
-
Evaluating the dosimetric impact of deep-learning-based auto-segmentation in prostate cancer radiotherapy: Insights into real-world clinical implementation and inter-observer variability.J Appl Clin Med Phys. 2025 Mar;26(3):e14569. doi: 10.1002/acm2.14569. Epub 2024 Dec 1. J Appl Clin Med Phys. 2025. PMID: 39616629 Free PMC article.
-
Comparison of commercial atlas-based automatic segmentation software for prostate radiotherapy treatment planning.Phys Eng Sci Med. 2024 Sep;47(3):881-894. doi: 10.1007/s13246-024-01411-2. Epub 2024 Apr 22. Phys Eng Sci Med. 2024. PMID: 38647633
-
A pair of deep learning auto-contouring models for prostate cancer patients injected with a radio-transparent versus radiopaque hydrogel spacer.Med Phys. 2023 Jun;50(6):3324-3337. doi: 10.1002/mp.16375. Epub 2023 Mar 24. Med Phys. 2023. PMID: 36940384
-
Development of Prostate Bed Delineation Consensus Guidelines for Magnetic Resonance Image-Guided Radiotherapy and Assessment of Its Effect on Interobserver Variability.Int J Radiat Oncol Biol Phys. 2024 Feb 1;118(2):378-389. doi: 10.1016/j.ijrobp.2023.08.051. Epub 2023 Aug 25. Int J Radiat Oncol Biol Phys. 2024. PMID: 37633499 Review.
-
Pelvic normal tissue contouring guidelines for radiation therapy: a Radiation Therapy Oncology Group consensus panel atlas.Int J Radiat Oncol Biol Phys. 2012 Jul 1;83(3):e353-62. doi: 10.1016/j.ijrobp.2012.01.023. Epub 2012 Apr 6. Int J Radiat Oncol Biol Phys. 2012. PMID: 22483697 Free PMC article.
Cited by
-
Autosegmentation based on different-sized training datasets of consistently-curated volumes and impact on rectal contours in prostate cancer radiation therapy.Phys Imaging Radiat Oncol. 2022 May 5;22:67-72. doi: 10.1016/j.phro.2022.04.007. eCollection 2022 Apr. Phys Imaging Radiat Oncol. 2022. PMID: 35572041 Free PMC article.
-
Automatic image segmentation based on synthetic tissue model for delineating organs at risk in spinal metastasis treatment planning.Strahlenther Onkol. 2019 Dec;195(12):1094-1103. doi: 10.1007/s00066-019-01463-4. Epub 2019 Apr 29. Strahlenther Onkol. 2019. PMID: 31037351 Free PMC article.
-
Automated Contouring and Planning in Radiation Therapy: What Is 'Clinically Acceptable'?Diagnostics (Basel). 2023 Feb 10;13(4):667. doi: 10.3390/diagnostics13040667. Diagnostics (Basel). 2023. PMID: 36832155 Free PMC article. Review.
-
Multicentre evaluation of deep learning CT autosegmentation of the head and neck region for radiotherapy.NPJ Digit Med. 2025 May 27;8(1):312. doi: 10.1038/s41746-025-01624-z. NPJ Digit Med. 2025. PMID: 40419731 Free PMC article.
-
Dosimetric comparison of automatically propagated prostate contours with manually drawn contours in MRI-guided radiotherapy: A step towards a contouring free workflow?Clin Transl Radiat Oncol. 2022 Aug 6;37:25-32. doi: 10.1016/j.ctro.2022.08.004. eCollection 2022 Nov. Clin Transl Radiat Oncol. 2022. PMID: 36052018 Free PMC article.
References
-
- Michalski JM, Lawton C, El Naqa I, Ritter M, O'Meara E, Seider MJ, Lee WR, Rosenthal SA, Pisansky T, Catton C. et al.Development of RTOG consensus guidelines for the definition of the clinical target volume for postoperative conformal radiation therapy for prostate cancer. Int J Radiat Oncol Biol Phys. 2010;76(2):361–368. doi: 10.1016/j.ijrobp.2009.02.006. - DOI - PMC - PubMed
-
- Wiltshire KL, Brock KK, Haider MA, Zwahlen D, Kong V, Chan E, Moseley J, Bayley A, Catton C, Chung PW. et al.Anatomic boundaries of the clinical target volume (prostate bed) after radical prostatectomy. Int J Radiat Oncol Biol Phys. 2007;69(4):1090–1099. doi: 10.1016/j.ijrobp.2007.04.068. - DOI - PubMed
-
- Mitchell DM, Perry L, Smith S, Elliott T, Wylie JP, Cowan RA, Livsey JE, Logue JP. Assessing the effect of a contouring protocol on postprostatectomy radiotherapy clinical target volumes and interphysician variation. Int J Radiat Oncol Biol Phys. 2009;75(4):990–993. doi: 10.1016/j.ijrobp.2008.12.042. - DOI - PubMed
-
- Lawton CA, Michalski J, El-Naqa I, Kuban D, Lee WR, Rosenthal SA, Zietman A, Sandler H, Shipley W, Ritter M. et al.Variation in the definition of clinical target volumes for pelvic nodal conformal radiation therapy for prostate cancer. Int J Radiat Oncol Biol Phys. 2009;74(2):377–382. doi: 10.1016/j.ijrobp.2008.08.003. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
