

Factors associated with default from treatment among tuberculosis patients in Nairobi province, Kenya: a case control study
- PMID: 21906291
- PMCID: PMC3224095
- DOI: 10.1186/1471-2458-11-696
Factors associated with default from treatment among tuberculosis patients in Nairobi province, Kenya: a case control study
Abstract
Background: Successful treatment of tuberculosis (TB) involves taking anti-tuberculosis drugs for at least six months. Poor adherence to treatment means patients remain infectious for longer, are more likely to relapse or succumb to tuberculosis and could result in treatment failure as well as foster emergence of drug resistant tuberculosis. Kenya is among countries with high tuberculosis burden globally. The purpose of this study was to determine the duration tuberculosis patients stay in treatment before defaulting and factors associated with default in Nairobi.
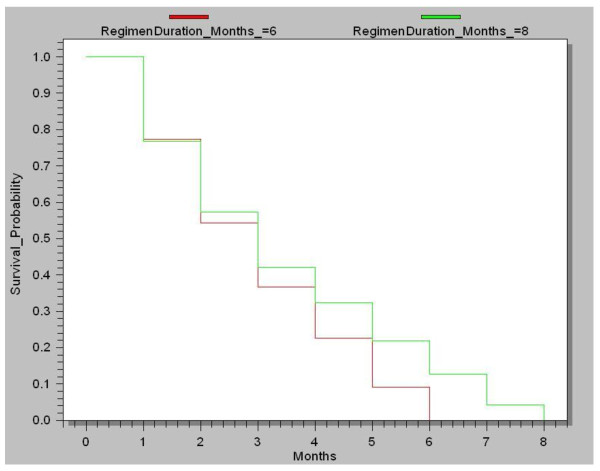
Methods: A Case-Control study; Cases were those who defaulted from treatment and Controls those who completed treatment course between January 2006 and March 2008. All (945) defaulters and 1033 randomly selected controls from among 5659 patients who completed treatment course in 30 high volume sites were enrolled. Secondary data was collected using a facility questionnaire. From among the enrolled, 120 cases and 154 controls were randomly selected and interviewed to obtain primary data not routinely collected. Data was analyzed using SPSS and Epi Info statistical software. Univariate and multivariate logistic regression analysis to determine association and Kaplan-Meier method to determine probability of staying in treatment over time were applied.
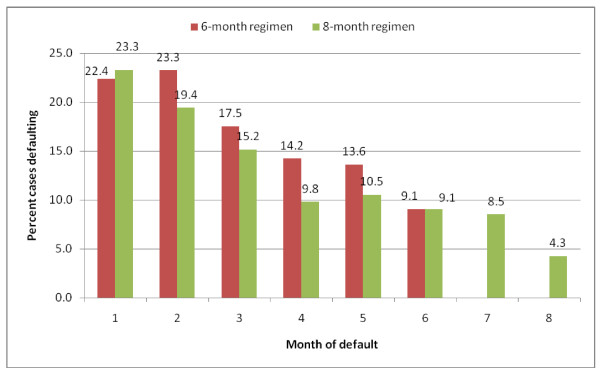
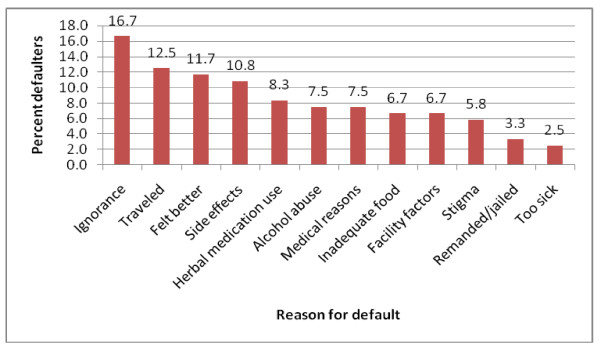
Results: Of 945 defaulters, 22.7% (215) and 20.4% (193) abandoned treatment within first and second months (intensive phase) of treatment respectively. Among 120 defaulters interviewed, 16.7% (20) attributed their default to ignorance, 12.5% (15) to traveling away from treatment site, 11.7% (14) to feeling better and 10.8% (13) to side-effects. On multivariate analysis, inadequate knowledge on tuberculosis (OR 8.67; 95% CI 1.47-51.3), herbal medication use (OR 5.7; 95% CI 1.37-23.7), low income (OR 5.57, CI 1.07-30.0), alcohol abuse (OR 4.97; 95% CI 1.56-15.9), previous default (OR 2.33; 95% CI 1.16-4.68), co-infection with Human immune-deficient Virus (HIV) (OR 1.56; 95% CI 1.25-1.94) and male gender (OR 1.43; 95% CI 1.15-1.78) were independently associated with default.
Conclusion: The rate of defaulting was highest during initial two months, the intensive phase of treatment. Multiple factors were attributed by defaulting patients as cause for abandoning treatment whereas several were independently associated with default. Enhanced patient pre-treatment counseling and education about TB is recommended.
Figures
References
-
- Hong Kong Chest Service/British Medical Research Council. Controlled trial of 2, 4, and 6 months of pyrazinamide in 6-month three times weekly regimens for smear-positive pulmonary tuberculosis, including an assessment of a combined preparation of isoniazid, rifampin and pyrazinamide: results at 30 months. Am Rev Respir Dis. 1991;143:700–706. - PubMed
-
- Jakubowiak WM, Bogorodskaya EW, Borisov ES, Danilova DI, Kourbatova EK. Risk factors associated with default among new pulmonary TB patients and social support in six Russian regions. The International Journal of TB and Lung Disease. 2007;11(1):46–53. - PubMed
-
- WHO. Global tuberculosis control, surveillance, planning, financing report. 2008.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
