

Corticosteroids for severe sepsis: an evidence-based guide for physicians
- PMID: 21906332
- PMCID: PMC3224490
- DOI: 10.1186/2110-5820-1-7
Corticosteroids for severe sepsis: an evidence-based guide for physicians
Abstract
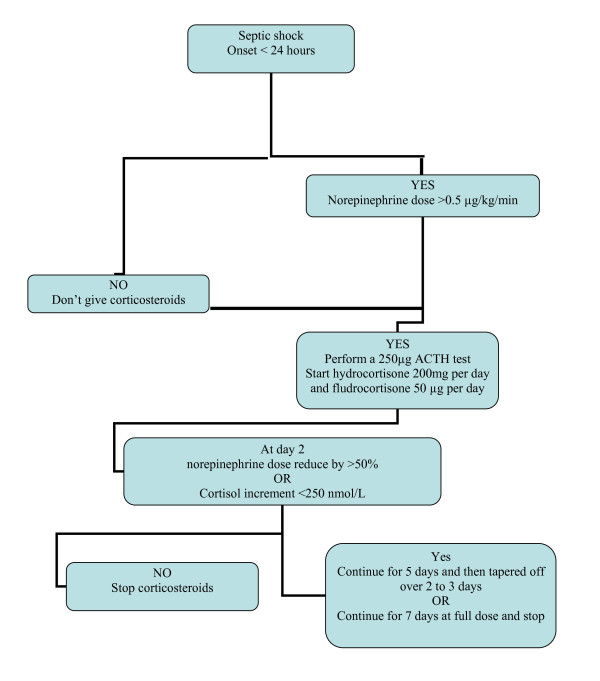
Septic shock is characterized by uncontrolled systemic inflammation that contributes to the progression of organ failures and eventually death. There is now ample evidence that the inability of the host to mount an appropriate hypothalamic-pituitary and adrenal axis response plays a major in overwhelming systemic inflammation during infections. Proinflammatory mediators released in the inflamed sites oppose to the anti-inflammatory response, an effect that may be reversed by exogenous corticosteroids. With sepsis, via nongenomic and genomic effects, corticosteroids restore cardiovascular homeostasis, terminate systemic and tissue inflammation, restore organ function, and prevent death. These effects of corticosteroids have been consistently found in animal studies and in most recent frequentist and Bayesian meta-analyses. Corticosteroids should be initiated only in patients with sepsis who require 0.5 μg/kg per minute or more of norepinephrine and should be continued for 5 to 7 days except in patients with poor hemodynamic response after 2 days of corticosteroids and with a cortisol increment of more than 250 nmol/L after a standard adrenocorticotropin hormone (ACTH) test. Hydrocortisone should be given at a daily dose of 200 mg and preferably combined to enteral fludrocortisone at a dose of 50 μg. Blood glucose levels should be kept below 150 mg/dL.
Figures
References
-
- Chrousos GP. The hypothalamic-pituitary-adrenal axis and immune-mediated inflammation. N Engl J Med. 1995;322(20):1351–1362. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
