

Management of neurological complications of infective endocarditis in ICU patients
- PMID: 21906336
- PMCID: PMC3224466
- DOI: 10.1186/2110-5820-1-10
Management of neurological complications of infective endocarditis in ICU patients
Abstract
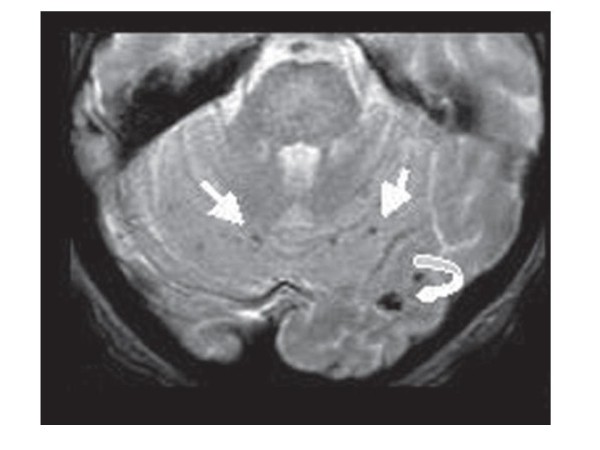
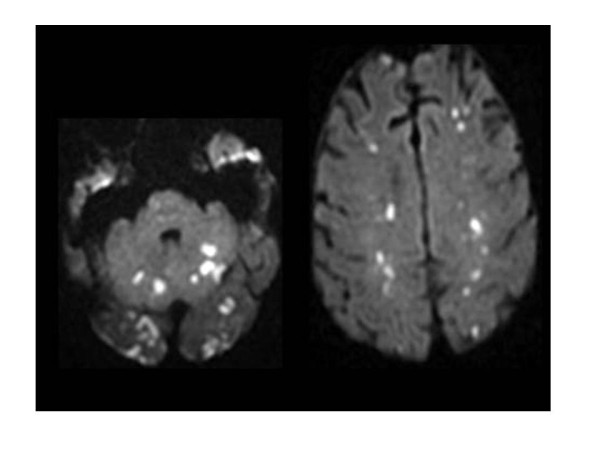
Patients with infective endocarditis (IE) are generally referred to the intensive care unit (ICU) for one or more organ dysfunctions caused by complications of IE. Neurologic events are frequent causes of ICU admission in patients with IE. They can arise through various mechanisms consisting of stroke or transient ischemic attack, cerebral hemorrhage, mycotic aneurysm, meningitis, cerebral abscess, or encephalopathy. Most complications occur early during the course of IE and are a hallmark of left-sided abnormalities of native or prosthetic valves. Occlusion of cerebral arteries, with stroke or transient ischemic attack, accounts for 40% to 50% of the central nervous system complications of IE. CT scan is the most easily feasible neuroimaging in critically unstable patients. However, magnetic resonance imaging is more sensitive and when performed should follow a standardized protocol. In patients with ischemic stroke who are already receiving oral anticoagulant therapy, this treatment should be replaced by unfractionated heparin for at least 2 weeks with a close monitoring of coagulation tests. Mounting evidence shows that, for both complicated left-sided native valve endocarditis and Staphylococcus aureus prosthetic valve endocarditis, valve replacement combined with medical therapy is associated with a better outcome than medical treatment alone. In a recent series, approximately 50% of patients underwent valve replacement during the acute phase of IE before completion of antibiotic treatment. After a neurological event, most patients have at least one indication for cardiac surgery. Recent data from literature suggest that after a stroke, surgery indicated for heart failure, uncontrolled infection, abscess, or persisting high emboli risk should not be delayed, provided that the patient is not comatose or has no severe deficit. Neurologic complications of IE contribute to a severe prognosis in ICU patients. However, patients with only silent or transient stroke had a better prognosis than patients with symptomatic events. In addition, more than neurologic event per se, a better predictor of mortality is neurologic dysfunction, which is associated with location and extension of brain damage. Patients with severe neurological impairment and those with brain hemorrhage have the worse outcome.
Figures
References
-
- Pankey GA. Subacute bacterial endocarditis at the University of Minnesota Hospital, 1939 through 1959. Ann Intern Med. 1961;55:550–561. - PubMed
-
- Francioli P. In: Infections of the Central Nervous System. Scheld WM, Whitley RJ, Durack DT, editor. Philadelphia: Lippincott-Raven; 1997. Complications of infective endocarditis; pp. 523–553.
-
- Heiro M, Nikoskelainen J, Engblom E, Kotilainen E, Marttila R, Kotilainen P. Association pour l' Etude et la Prévention de l' Endocardite Infectieuse (AEPEI) Study Group. Neurologic manifestations of infective endocarditis: a 17-year experience in a teaching hospital in Finland. Arch Intern Med. 2000;160:2781–2787. doi: 10.1001/archinte.160.18.2781. - DOI - PubMed
-
- Hoen B, Alla F, Selton-Suty C, Bouvet A, Briançon S, Casalta JP, Danchin N, Delahaye F, Etienne J, Le Moing V, Leport C, Mainardi JL, Ruimy R, Vandenesch F. Changing profile of infective endocarditis: results of a 1-year survey in France. JAMA. 2002;288:75–81. doi: 10.1001/jama.288.1.75. - DOI - PubMed
LinkOut - more resources
Full Text Sources
