

MRP8 and MRP14, phagocyte-specific danger signals, are sensitive biomarkers of disease activity in cryopyrin-associated periodic syndromes
- PMID: 21908452
- PMCID: PMC4174360
- DOI: 10.1136/ard.2011.152496
MRP8 and MRP14, phagocyte-specific danger signals, are sensitive biomarkers of disease activity in cryopyrin-associated periodic syndromes
Abstract
Objectives: To assess the sensitivity of the phagocyte-specific molecules myeloid-related protein (MRP) 8 and MRP14 (calprotectin) for monitoring disease activity during anti-interleukin (IL)-1 therapies in patients with cryopyrin-associated periodic syndromes (CAPS), including familial cold autoinflammatory syndrome (FCAS), Muckle-Wells syndrome (MWS) and chronic infantile neurological, cutaneous and articular (CINCA) syndrome.
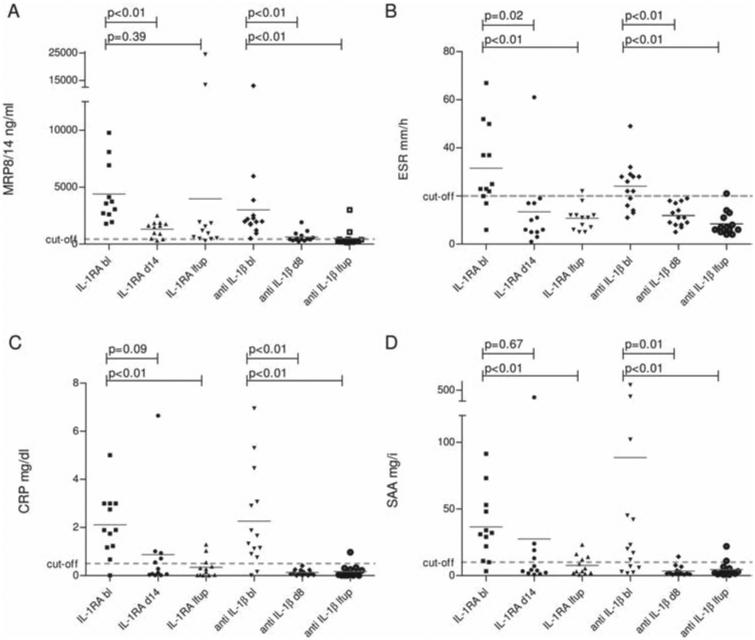
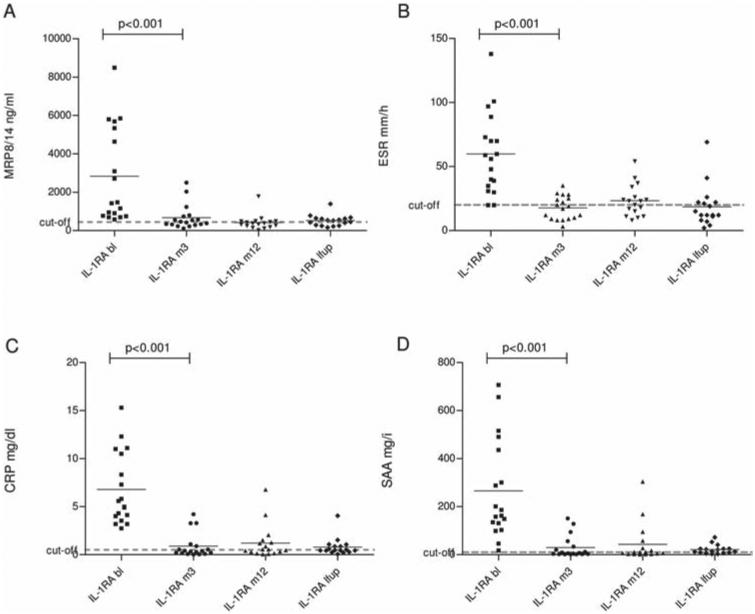
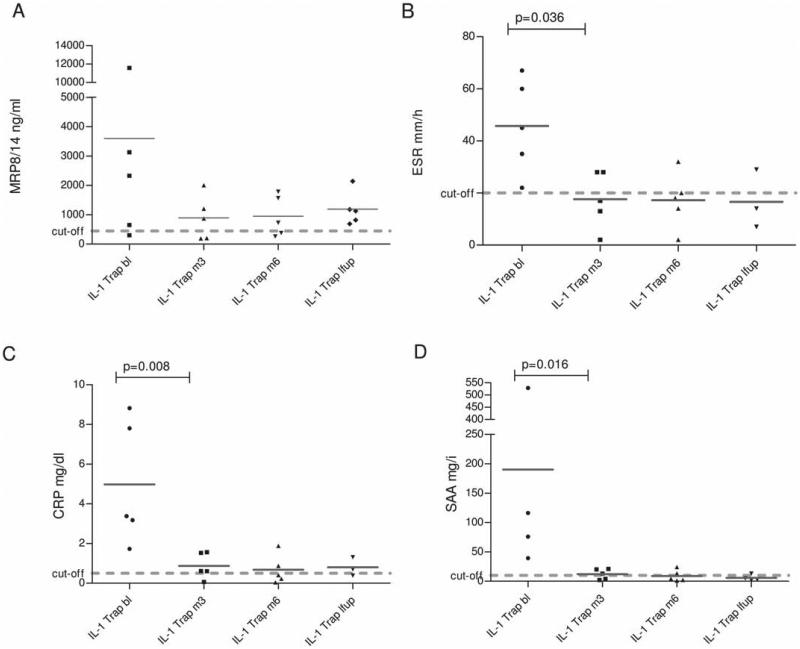
Methods: A total of 39 patients with CAPS, including 5 FCAS, 16 MWS and 18 CINCA syndrome, received anti-IL-1 therapy. All patients with CINCA and 12 with MWS were treated with IL-1Ra (anakinra), 14 patients with MWS with a monoclonal anti-IL-1β antibody (canakinumab) and patients with FCAS received IL-1 Trap (rilonacept). During serial clinical visits serum amyloid A, C-reactive protein, erythrocyte sedimentation rate and MRP8/14 serum levels were analysed.
Results: Untreated patients with CAPS had significantly elevated MRP8/14 values. In response to treatment there was a significant reduction of MRP8/14 levels in CINCA (2,830 (range 690 - 8,480) ng/ml to 670 ng/ml, p < 0.001) and MWS patients (anakinra-treated: 4,390 (1790 - 9780) ng/ml to 1,315 ng/ml (p = 0.003); canakinumab-treated: 3,000 (500 - 13060) ng/ml to 630 ng/ml (p=0.001)). However, in many patients with CAPS, MRP8/14 levels were still elevated compared with healthy individuals, reflecting residual disease activity. However, canakinumab-treated patients with CAPS showed normalised MRP8/14 levels, suggesting control of phagocyte activation.
Conclusions: Monitoring of cellular systems involved in inflammatory cascades of the innate immunity was successfully applied to the IL-1-driven CAPS diseases. This is the first study illustrating different states of subclinical disease activity in all types of CAPS depending on the type of anti-IL-1 therapy. MRP8/14 is a sensitive biomarker for monitoring disease activity, status of inflammation and response to IL-1 blockade in patients with CAPS.
Figures
References
-
- Kanneganti TD, Ozören N, Body-Malapel M, et al. Bacterial RNA and small antiviral compounds activate caspase-1 through cryopyrin/Nalp3. Nature. 2006;440:233–6. - PubMed
-
- Mariathasan S, Weiss DS, Newton K, et al. Cryopyrin activates the inflammasome in response to toxins and ATP. Nature. 2006;440:228–32. - PubMed
-
- Martinon F, Pétrilli V, Mayor A, et al. Gout-associated uric acid crystals activate the NALP3 inflammasome. Nature. 2006;440:237–41. - PubMed
-
- Sutterwala FS, Ogura Y, Szczepanik M, et al. Critical role for NALP3/CIAS1/Cryopyrin in innate and adaptive immunity through its regulation of caspase-1. Immunity. 2006;24:317–27. - PubMed
-
- Agostini L, Martinon F, Burns K, et al. NALP3 forms an IL-1beta-processing inflammasome with increased activity in Muckle-Wells autoinflammatory disorder. Immunity. 2004;20:319–25. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
