

Clinical and neuroanatomical signatures of tissue pathology in frontotemporal lobar degeneration
- PMID: 21908872
- PMCID: PMC3170537
- DOI: 10.1093/brain/awr198
Clinical and neuroanatomical signatures of tissue pathology in frontotemporal lobar degeneration
Abstract
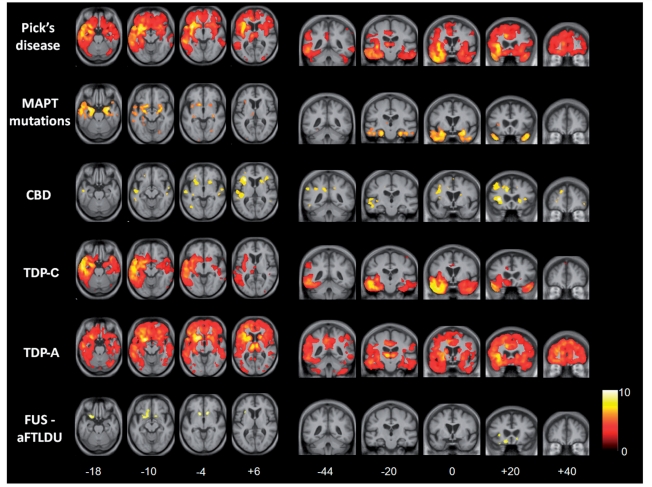
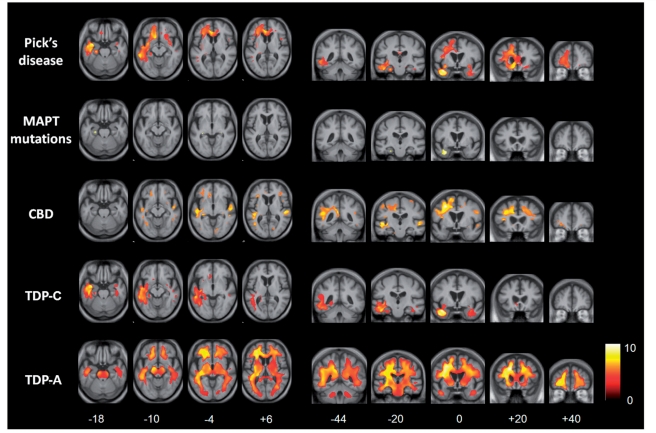
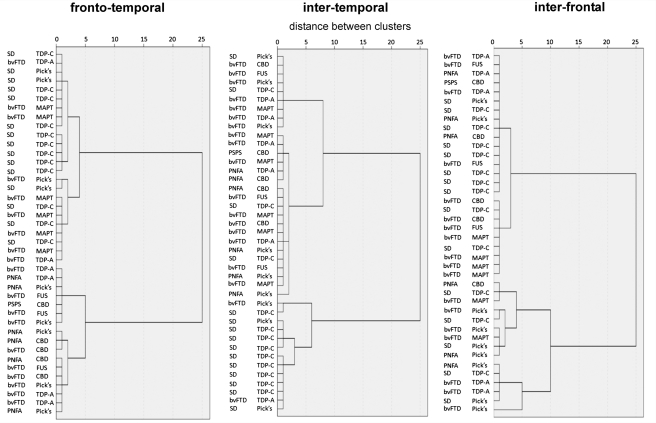
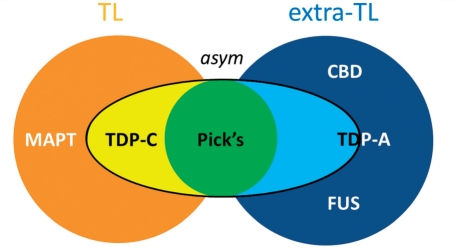
Relating clinical symptoms to neuroanatomical profiles of brain damage and ultimately to tissue pathology is a key challenge in the field of neurodegenerative disease and particularly relevant to the heterogeneous disorders that comprise the frontotemporal lobar degeneration spectrum. Here we present a retrospective analysis of clinical, neuropsychological and neuroimaging (volumetric and voxel-based morphometric) features in a pathologically ascertained cohort of 95 cases of frontotemporal lobar degeneration classified according to contemporary neuropathological criteria. Forty-eight cases (51%) had TDP-43 pathology, 42 (44%) had tau pathology and five (5%) had fused-in-sarcoma pathology. Certain relatively specific clinicopathological associations were identified. Semantic dementia was predominantly associated with TDP-43 type C pathology; frontotemporal dementia and motoneuron disease with TDP-43 type B pathology; young-onset behavioural variant frontotemporal dementia with FUS pathology; and the progressive supranuclear palsy syndrome with progressive supranuclear palsy pathology. Progressive non-fluent aphasia was most commonly associated with tau pathology. However, the most common clinical syndrome (behavioural variant frontotemporal dementia) was pathologically heterogeneous; while pathologically proven Pick's disease and corticobasal degeneration were clinically heterogeneous, and TDP-43 type A pathology was associated with similar clinical features in cases with and without progranulin mutations. Volumetric magnetic resonance imaging, voxel-based morphometry and cluster analyses of the pathological groups here suggested a neuroanatomical framework underpinning this clinical and pathological diversity. Frontotemporal lobar degeneration-associated pathologies segregated based on their cerebral atrophy profiles, according to the following scheme: asymmetric, relatively localized (predominantly temporal lobe) atrophy (TDP-43 type C); relatively symmetric, relatively localized (predominantly temporal lobe) atrophy (microtubule-associated protein tau mutations); strongly asymmetric, distributed atrophy (Pick's disease); relatively symmetric, predominantly extratemporal atrophy (corticobasal degeneration, fused-in-sarcoma pathology). TDP-43 type A pathology was associated with substantial individual variation; however, within this group progranulin mutations were associated with strongly asymmetric, distributed hemispheric atrophy. We interpret the findings in terms of emerging network models of neurodegenerative disease: the neuroanatomical specificity of particular frontotemporal lobar degeneration pathologies may depend on an interaction of disease-specific and network-specific factors.
Figures

Comment in
-
Sense and sensitivity of novel criteria for frontotemporal dementia.Brain. 2011 Sep;134(Pt 9):2450-3. doi: 10.1093/brain/awr208. Epub 2011 Aug 22. Brain. 2011. PMID: 21859764 No abstract available.
References
-
- Acosta-Cabronero J, Patterson K, Fryer TD, Hodges JR, Pengas G, Williams GB, et al. Atrophy, hypometabolism and white matter abnormalities in semantic dementia tell a coherent story. Brain. 2011;134(Pt 7):2025–35. - PubMed
-
- Alzheimer A. Uber eigenartige Krankheitsfalle des Spateren Alters. Z Ges Neurol Psychiatr. 1911;4:356–85.
-
- Boeve BF, Lang AE, Litvan I. Corticobasal degeneration and its relationship to progressive supranuclear palsy and frontotemporal dementia. Ann Neurol. 2003;54(Suppl. 5):S15–9. - PubMed
-
- Cairns NJ, Bigio EH, Mackenzie IR, Neumann M, Lee VM, Hatanpaa KJ, et al. Consortium for Frontotemporal Lobar Degeneration. Neuropathologic diagnostic and nosologic criteria for frontotemporal lobar degeneration: consensus of the Consortium for Frontotemporal Lobar Degeneration. Acta Neuropathol. 2007;114:5–22. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
