

Diffuse retinal injury from a non-penetrating TASER dart
- PMID: 21909993
- PMCID: PMC3214995
- DOI: 10.1007/s10633-011-9287-9
Diffuse retinal injury from a non-penetrating TASER dart
Abstract
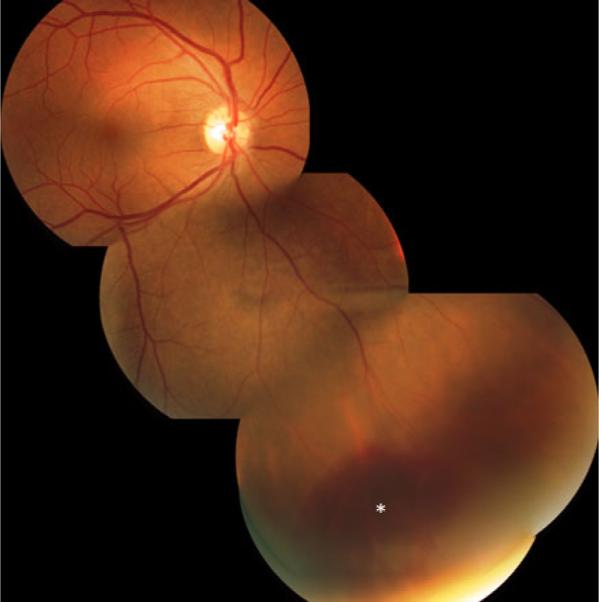
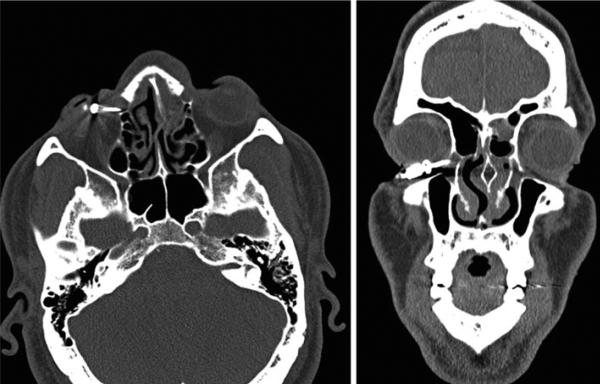
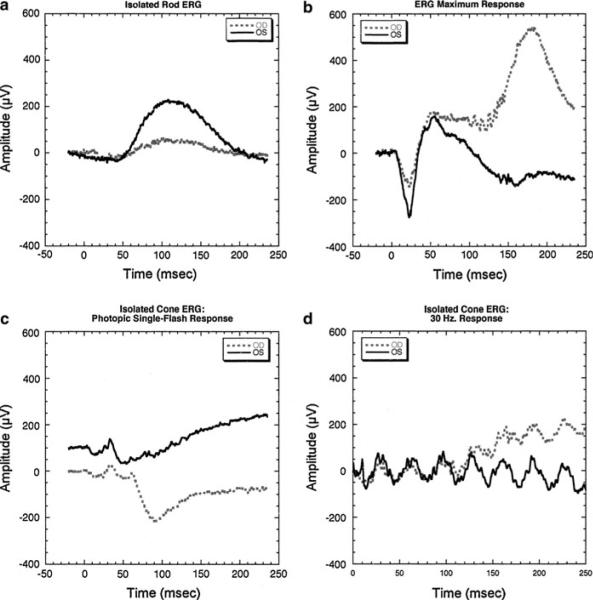
To describe a non-penetrating TASER gun injury resulting in a small exudative retinal detachment but significant visual acuity and retinal function loss as demonstrated by electroretinography (ERG). A 39-year-old man presented to the emergency department with a TASER barb embedded in his right lower lid. A complete clinical ophthalmologic examination and surgical extrication were performed, as well as radiologic imaging and Ganzfeld electroretinography. No scleral penetration was observed on surgical exploration. Retinal examination showed a peripheral exudative detachment. Subsequent follow-up revealed progressive resolution of the detachment and improvement in visual acuity. The ERG showed a 63-70% decrease in rod a- and b-waves, while isolated cone responses were reduced by only 10%, with a minimal increase in implicit time. This case shows that periocular TASER injuries, even if apparently superficial, may result in significant ocular damage. ERG may be useful in the diagnosis of visual loss attributed to disturbance in photoreceptor function, in the absence of anatomically evident damage.
Figures


References
-
- TASER promotional literature. http://taser.com/products/personal-safety/taser-c2. Accessed 1 May 2009.
-
- Bozeman WP, Hauda WE, II, Heck JJ, Graham DD, Jr, Martin BP, Winslow JE. Safety and injury profile of conducted electrical weapons used by law enforcement officers against criminal suspects. Ann Emerg Med. 2009;53:480–489. - PubMed
-
- Marmor MF, Fulton AB, Holder GE, Miyake Y, Brigell M, Bach M. ISCEV Standard for full-field clinical electroretinography (2008 update) Doc Ophthalmol. 2009;118:69–77. - PubMed
-
- Seth RK, Abedi G, Daccache AJ, Tsai JC. Cataract secondary to electrical shock from a Taser gun. J Cataract Refract Surg. 2007;33:1664–1665. - PubMed
-
- Teymoorian S, San Filippo AN, Poulose AK, Lyon DB. Perforating globe injury from Taser trauma. Ophthal Plast Reconstr Surg. 2010;26:306–308. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
