

Early postoperative outcomes and blood product utilization in adult cardiac surgery: the post-aprotinin era
- PMID: 21911820
- PMCID: PMC3181091
- DOI: 10.1161/CIRCULATIONAHA.110.002543
Early postoperative outcomes and blood product utilization in adult cardiac surgery: the post-aprotinin era
Abstract
Background: Aprotinin was a commonly used pharmacological agent for homeostasis in cardiac surgery but was discontinued, resulting in the extensive use of lysine analogues. This study tested the hypothesis that early postoperative adverse events and blood product utilization would affected in this post-aprotinin era.
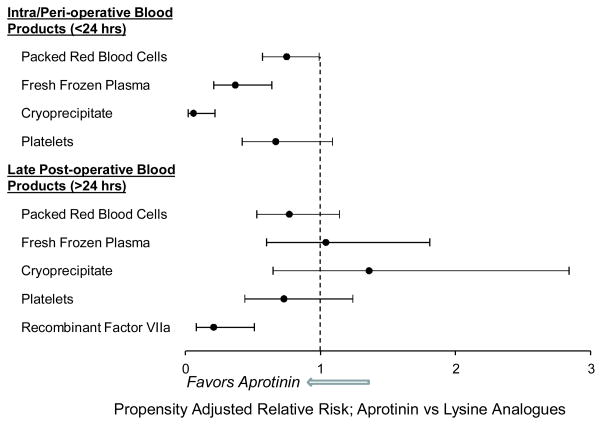
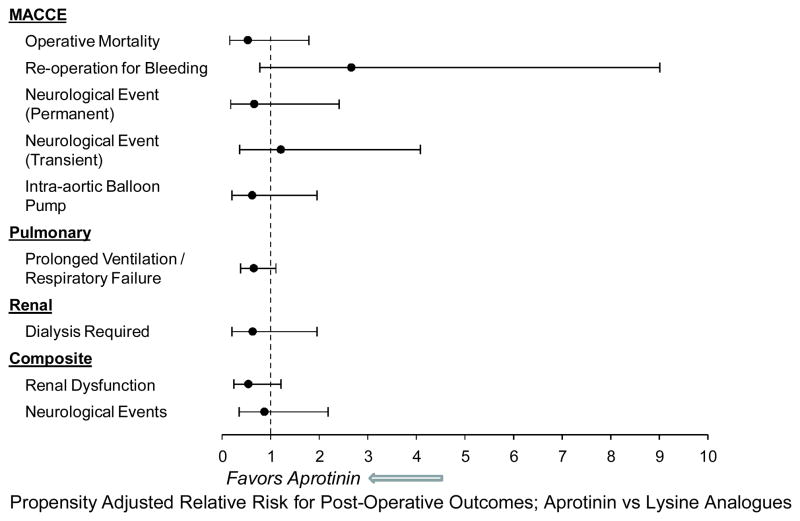
Methods and results: Adult patients (n=781) undergoing coronary artery bypass, valve replacement, or both from November 1, 2005, to October 31, 2008, at a single institution were included. Multiple logistic regression modeling and propensity scoring were performed on 29 preoperative and intraoperative variables in patients receiving aprotinin (n=325) or lysine analogues (n=456). The propensity-adjusted relative risk (RR) for the intraoperative use of packed red blood cells (RR, 0.75; 95% confidence interval [CI], 0.57 to 0.99), fresh frozen plasma (RR, 0.37; 95% CI, 0.21 to 0.64), and cryoprecipitate (RR:0.06; 95% CI, 0.02 to 0.22) were lower in the aprotinin versus lysine analog group (all P<0.05). The risk for mortality (RR, 0.53; 95% CI, 0.16 to 1.79) and neurological events (RR, 0.87; 95% CI, 0.35 to 2.18) remained similar between groups, whereas a trend for reduced risk for renal dysfunction was observed in the aprotinin group.
Conclusions: In the post-aprotinin era, with the exclusive use of lysine analogues, the relative risk of early postoperative outcomes such as mortality and renal dysfunction have not improved, but the risk for the intraoperative use of blood products has increased. Thus, improvements in early postoperative outcomes have not been realized with the discontinued use of aprotinin, but rather increased blood product use has occurred with the attendant costs and risks inherent with this strategy.
Figures
References
-
- Sedrakyan A, Treasure T, Elefteriades JA. Effect of aprotinin on clinical outcomes in coronary artery bypass graft surgery: a systematic review and meta-analysis of randomized clinical trials. J Thorac Cardiovasc Surg. 2004;128:442–8. - PubMed
-
- Levi M, Cromheecke ME, de Jonge E, Prins MH, de Mol BJ, Briët E, Büller HR. Pharmacological strategies to decrease excessive blood loss in cardiac surgery: a meta-analysis of clinically relevant endpoints. Lancet. 1999;354:1940–7. - PubMed
-
- Brown JR, Birkmeyer NJ, O’Connor GT. Meta-analysis comparing the effectiveness and adverse outcomes of antifibrinolytic agents in cardiac surgery. Circulation. 2007;115:2801–13. - PubMed
-
- Kristeller JL, Roslund BP, Stahl RF. Benefits and risks of aprotinin use during cardiac surgery. Pharmacotherapy. 2008;28:112–24. - PubMed
-
- Ngaage DL, Cale AR, Cowen ME, Griffin S, Guvendik L. Aprotinin in primary cardiac surgery: operative outcome of propensity score-matched study. Ann Thorac Surg. 2008;86:1195–202. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
