

Pregnancy, microchimerism, and the maternal grandmother
- PMID: 21912617
- PMCID: PMC3166068
- DOI: 10.1371/journal.pone.0024101
Pregnancy, microchimerism, and the maternal grandmother
Abstract
Background: A WOMAN OF REPRODUCTIVE AGE OFTEN HARBORS A SMALL NUMBER OF FOREIGN CELLS, REFERRED TO AS MICROCHIMERISM: a preexisting population of cells acquired during fetal life from her own mother, and newly acquired populations from her pregnancies. An intriguing question is whether the population of cells from her own mother can influence either maternal health during pregnancy and/or the next generation (grandchildren).
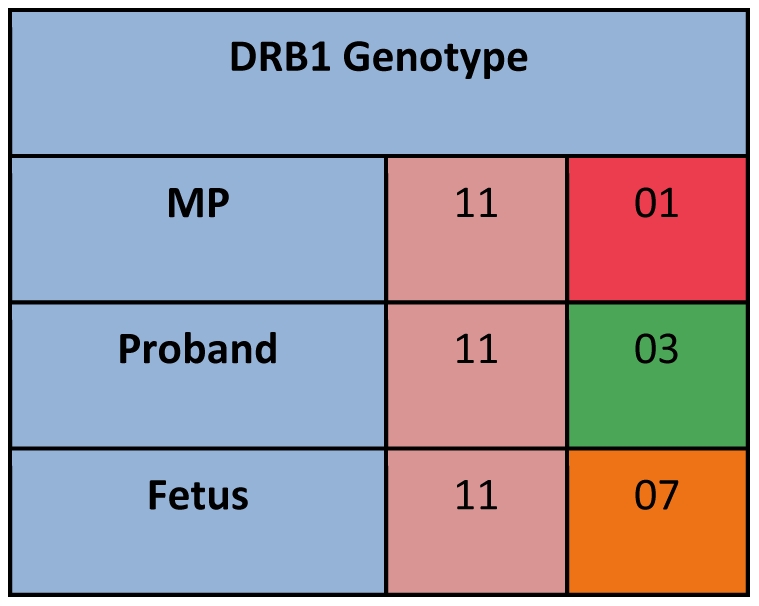
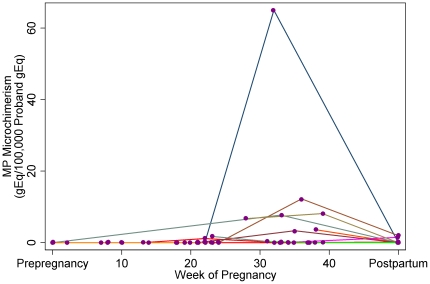
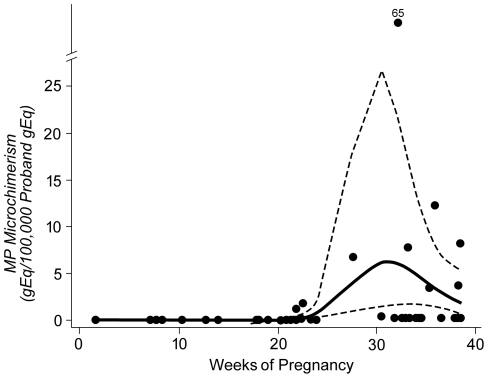
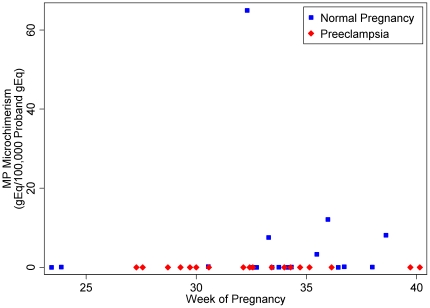
Methodology/principal findings: Microchimerism from a woman's (i.e. proband's) own mother (mother-of-the-proband, MP) was studied in peripheral blood samples from women followed longitudinally during pregnancy who were confirmed to have uncomplicated obstetric outcomes. Women with preeclampsia were studied at the time of diagnosis and comparison made to women with healthy pregnancies matched for parity and gestational age. Participants and family members were HLA-genotyped for DRB1, DQA1, and DQB1 loci. An HLA polymorphism unique to the woman's mother was identified, and a panel of HLA-specific quantitative PCR assays was employed to identify and quantify microchimerism. Microchimerism from the MP was identified during normal, uncomplicated pregnancy, with a peak concentration in the third trimester. The likelihood of detection increased with advancing gestational age. For each advancing trimester, there was a 12.7-fold increase in the probability of detecting microchimerism relative to the prior trimester, 95% confidence intervals 3.2, 50.3, p<0.001. None of the women with preeclampsia, compared with 30% of matched healthy women, had microchimerism (p = 0.03).
Conclusions/significance: These results show that microchimerism from a woman's own mother is detectable in normal pregnancy and diminished in preeclampsia, supporting the previously unexplored hypothesis that MP microchimerism may be a marker reflecting healthy maternal adaptation to pregnancy.
Conflict of interest statement
Figures
References
-
- van Rood JJ, Claas F. Both self and non-inherited maternal HLA antigens influence the immune response. Immunology Today. 2000;21:269–273. - PubMed
-
- Redman CWG, Sacks GP, Sargent IL. Preeclampsia: An excessive maternal inflammatory response to pregnancy. Am J Obstet Gynecol. 1999;180:499–506. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
