

Real-time PCR in HIV/Trypanosoma cruzi coinfection with and without Chagas disease reactivation: association with HIV viral load and CD4 level
- PMID: 21912712
- PMCID: PMC3166046
- DOI: 10.1371/journal.pntd.0001277
Real-time PCR in HIV/Trypanosoma cruzi coinfection with and without Chagas disease reactivation: association with HIV viral load and CD4 level
Abstract
Background: Reactivation of chronic Chagas disease, which occurs in approximately 20% of patients coinfected with HIV/Trypanosoma cruzi (T. cruzi), is commonly characterized by severe meningoencephalitis and myocarditis. The use of quantitative molecular tests to monitor Chagas disease reactivation was analyzed.
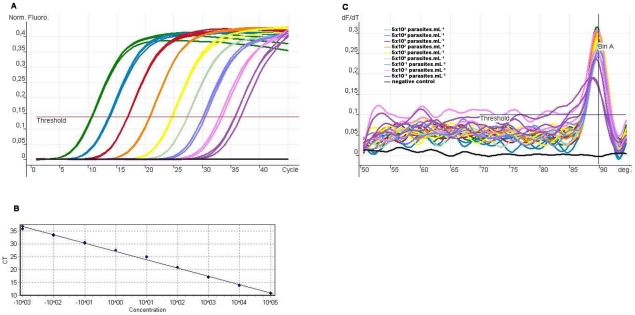
Methodology: Polymerase chain reaction (PCR) of kDNA sequences, competitive (C-) PCR and real-time quantitative (q) PCR were compared with blood cultures and xenodiagnosis in samples from 91 patients (57 patients with chronic Chagas disease and 34 with HIV/T. cruzi coinfection), of whom 5 had reactivation of Chagas disease and 29 did not.
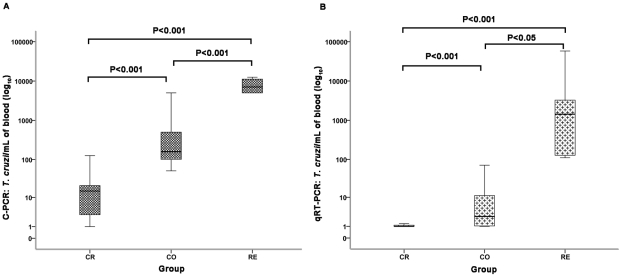
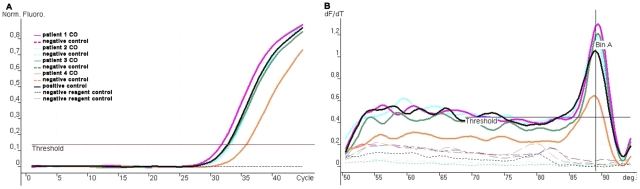
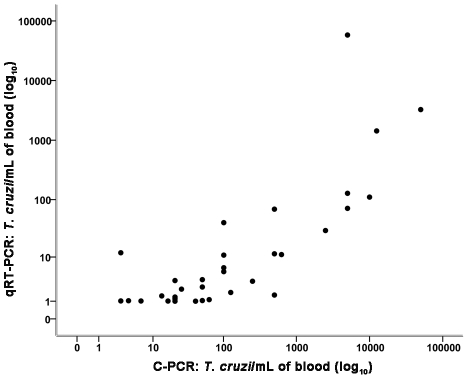
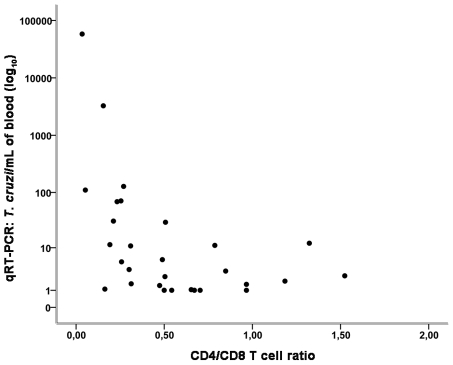
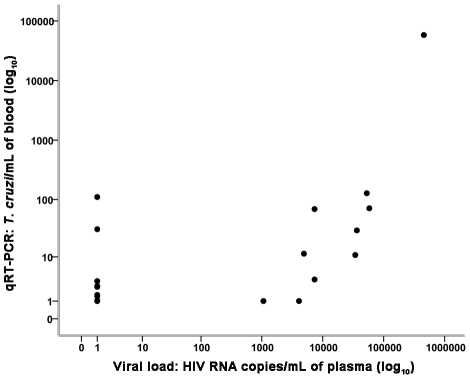
Principal findings: qRT-PCR showed significant differences between groups; the highest parasitemia was observed in patients infected with HIV/T. cruzi with Chagas disease reactivation (median 1428.90 T. cruzi/mL), followed by patients with HIV/T. cruzi infection without reactivation (median 1.57 T. cruzi/mL) and patients with Chagas disease without HIV (median 0.00 T. cruzi/mL). Spearman's correlation coefficient showed that xenodiagnosis was correlated with blood culture, C-PCR and qRT-PCR. A stronger Spearman correlation index was found between C-PCR and qRT-PCR, the number of parasites and the HIV viral load, expressed as the number of CD4(+) cells or the CD4(+)/CD8(+) ratio.
Conclusions: qRT-PCR distinguished the groups of HIV/T. cruzi coinfected patients with and without reactivation. Therefore, this new method of qRT-PCR is proposed as a tool for prospective studies to analyze the importance of parasitemia (persistent and/or increased) as a criterion for recommending pre-emptive therapy in patients with chronic Chagas disease with HIV infection or immunosuppression. As seen in this study, an increase in HIV viral load and decreases in the number of CD4(+) cells/mm(3) and the CD4(+)/CD8(+) ratio were identified as cofactors for increased parasitemia that can be used to target the introduction of early, pre-emptive therapy.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Weekly epidemiological record. Relevé épidémiologique hebdomadaire. No. 28/29. 2007;82:245–260.
-
- Fonseca MGP, Bastos FI. Twenty-five years of the AIDS epidemic in Brazil: principal epidemiological findings, 1980–2005. Cad Saúde Publica Rio de Janeiro. 2007;23(Suppl 3):S333–344. - PubMed
-
- Schmunis GA. Epidemiology of Chagas disease in non-endemic countries: the role of international migration. Mem Inst Osw Cruz. 2007;102(Suppl I):75–85. - PubMed
-
- CDC. Chagas disease after organ transplantation – Los Angeles, California, MMWR. 2006;55(29):798–800. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
