

Genetics of the HLA region in the prediction of type 1 diabetes
- PMID: 21912932
- PMCID: PMC3233362
- DOI: 10.1007/s11892-011-0223-x
Genetics of the HLA region in the prediction of type 1 diabetes
Abstract
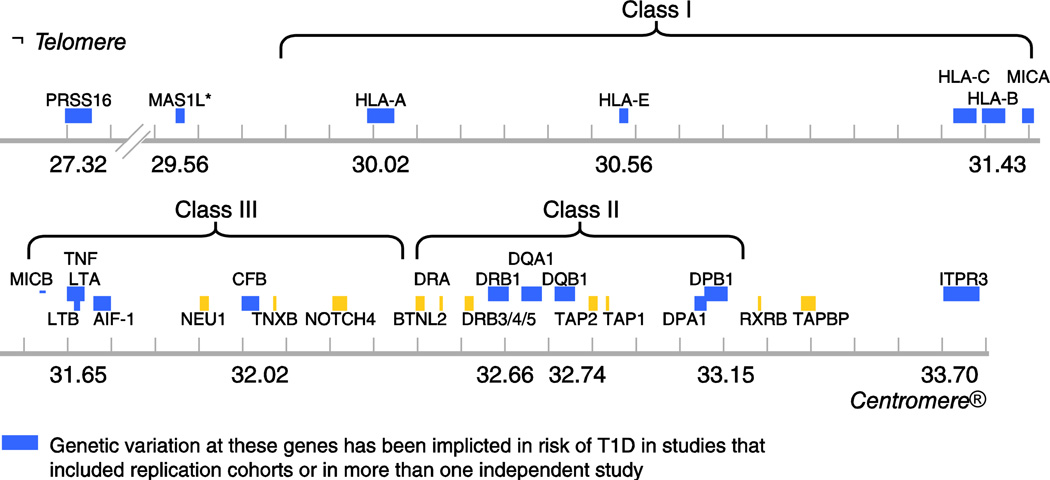
Type 1 diabetes (T1D) is one of the most widely studied complex genetic disorders, and the genes in HLA are reported to account for approximately 40-50% of the familial aggregation of T1D. The major genetic determinants of this disease are polymorphisms of class II HLA genes encoding DQ and DR. The DR-DQ haplotypes conferring the highest risk are DRB1*03:01-DQA1*05:01-DQB1*02:01 (abbreviated "DR3") and DRB1*04:01/02/04/05/08-DQA1*03:01-DQB1*03:02/04 (or DQB1*02; abbreviated "DR4"). The risk is much higher for the heterozygote formed by these two haplotypes (OR = 16.59; 95% CI, 13.7-20.1) than for either of the homozygotes (DR3/DR3, OR = 6.32; 95% CI, 5.12-7.80; DR4/DR4, OR = 5.68; 95% CI, 3.91). In addition, some haplotypes confer strong protection from disease, such as DRB1*15:01-DQA1*01:02-DQB1*06:02 (abbreviated "DR2"; OR = 0.03; 95% CI, 0.01-0.07). After adjusting for the genetic correlation with DR and DQ, significant associations can be seen for HLA class II DPB1 alleles, in particular, DPB1*04:02, DPB1*03:01, and DPB1*02:02. Outside of the class II region, the strongest susceptibility is conferred by class I allele B*39:06 (OR =10.31; 95% CI, 4.21-25.1) and other HLA-B alleles. In addition, several loci in the class III region are reported to be associated with T1D, as are some loci telomeric to class I. Not surprisingly, current approaches for the prediction of T1D in screening studies take advantage of genotyping HLA-DR and HLA-DQ loci, which is then combined with family history and screening for autoantibodies directed against islet-cell antigens. Inclusion of additional moderate HLA risk haplotypes may help identify the majority of children with T1D before the onset of the disease.
Conflict of interest statement
No potential conflicts of interest relevant to this article were reported.
Figures

References
-
-
Eisenbarth GS. Banting Lecture2009: An unfinished journey: molecular pathogenesis to prevention of type 1A diabetes. Diabetes. 2010;59:759–774. This lecture gives an excellent overview of T1D pathogenesis important to the understanding of the genetic susceptibility.
-
-
- Dunger DB, Sperling MA, Acerini CL, Bohn DJ, Daneman D, Danne TP, Glaser NS, Hanas R, Hintz RL, Levitsky LL, Savage MO, Tasker RC, Wolfsdorf JI. European Society for Paediatric Endocrinology/Lawson Wilkins Pediatric Endocrine Society consensus statement on diabetic ketoacidosis in children and adolescents. Pediatrics. 2004;113:e133–e140. - PubMed
-
- Karvonen M, Viik-Kajander M, Moltchanova E, Libman I, LaPorte R, Tuomilehto J. Incidence of childhood type 1 diabetes worldwide. Diabetes Mondiale (DiaMond) Project Group. Diabetes Care. 2000;23:1516–1526. - PubMed
-
- Dabelea D, Bell RA, D'Agostino RB, Jr, Imperatore G, Johansen JM, Linder B, Liu LL, Loots B, Marcovina S, Mayer-Davis EJ, Pettitt DJ, Waitzfelder B. Incidence of diabetes in youth in the United States. Jama. 2007;297:2716–2724. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
