

Ultrastructural differences between diabetic and idiopathic gastroparesis
- PMID: 21914127
- PMCID: PMC3250562
- DOI: 10.1111/j.1582-4934.2011.01451.x
Ultrastructural differences between diabetic and idiopathic gastroparesis
Abstract
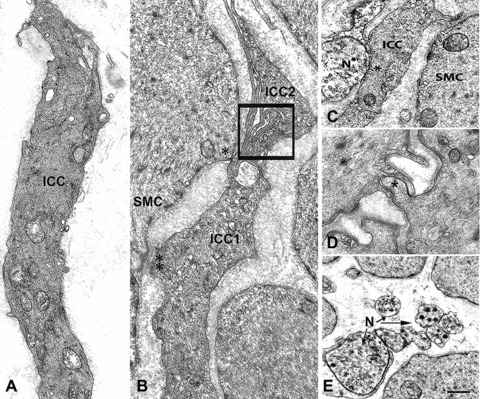
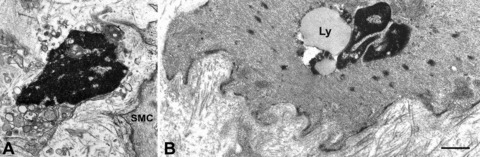
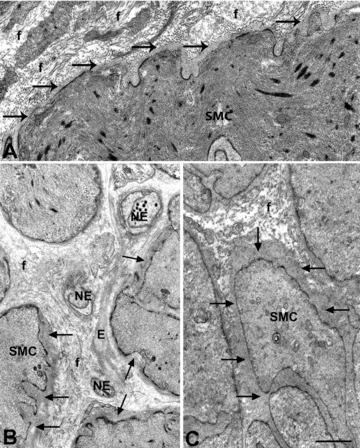
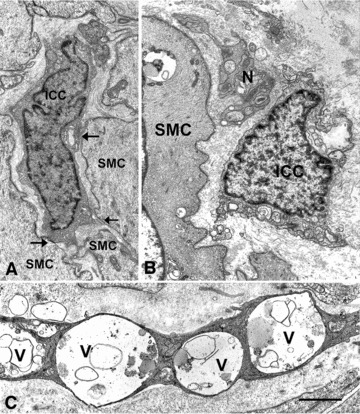
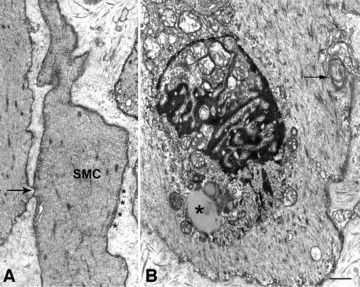
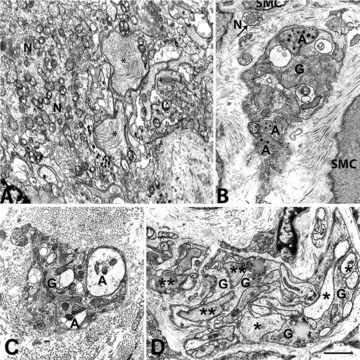
The ultrastructural changes in diabetic and idiopathic gastroparesis are not well studied and it is not known whether there are different defects in the two disorders. As part of the Gastroparesis Clinical Research Consortium, full thickness gastric body biopsies from 20 diabetic and 20 idiopathic gastroparetics were studied by light microscopy. Abnormalities were found in many (83%) but not all patients. Among the common defects were loss of interstitial cells of Cajal (ICC) and neural abnormalities. No distinguishing features were seen between diabetic and idiopathic gastroparesis. Our aim was to provide a detailed description of the ultrastructural abnormalities, compare findings between diabetic and idiopathic gastroparesis and determine if patients with apparently normal immunohistological features have ultrastructural abnormalities. Tissues from 40 gastroparetic patients and 24 age- and sex-matched controls were examined by transmission electron microscopy (TEM). Interstitial cells of Cajal showing changes suggestive of injury, large and empty nerve endings, presence of lipofuscin and lamellar bodies in the smooth muscle cells were found in all patients. However, the ultrastructural changes in ICC and nerves differed between diabetic and idiopathic gastroparesis and were more severe in idiopathic gastroparesis. A thickened basal lamina around smooth muscle cells and nerves was characteristic of diabetic gastroparesis whereas idiopathic gastroparetics had fibrosis, especially around the nerves. In conclusion, in all the patients TEM showed abnormalities in ICC, nerves and smooth muscle consistent with the delay in gastric emptying. The significant differences found between diabetic and idiopathic gastroparesis offers insight into pathophysiology as well as into potential targeted therapies.
© 2011 The Authors Journal of Cellular and Molecular Medicine © 2011 Foundation for Cellular and Molecular Medicine/Blackwell Publishing Ltd.
Figures



References
-
- Farrell FJ, Keeffe EB. Diabetic gastroparesis. Dig Dis. 1995;13:291–300. - PubMed
-
- Stanciu GO. Gastroparesis and its management. Rev Med Chir Soc Med Nat Iasi. 2001;105:451–6. - PubMed
-
- Horvath VJ, Vittal H, Lorincz A, et al. Reduced stem cell factor links smooth myopathy and loss of interstitial cells of Cajal in murine diabetic gastroparesis. Gastroenterology. 2006;130:759–70. - PubMed
-
- Ordog T, Takayama I, Cheung WK, et al. Remodeling of networks of interstitial cells of Cajal in a murine model of diabetic gastroparesis. Diabetes. 2000;49:1731–9. - PubMed
Publication types
MeSH terms
Grants and funding
- U01DK073975/DK/NIDDK NIH HHS/United States
- U01 DK074008/DK/NIDDK NIH HHS/United States
- R01 DK057061/DK/NIDDK NIH HHS/United States
- DK84567/DK/NIDDK NIH HHS/United States
- U01 DK073975/DK/NIDDK NIH HHS/United States
- U01 DK074035/DK/NIDDK NIH HHS/United States
- U01 DK073983/DK/NIDDK NIH HHS/United States
- U01DK074008/DK/NIDDK NIH HHS/United States
- U01DK073983/DK/NIDDK NIH HHS/United States
- U01DK073985/DK/NIDDK NIH HHS/United States
- U01DK073974/DK/NIDDK NIH HHS/United States
- P01 DK068055/DK/NIDDK NIH HHS/United States
- U01 DK074007/DK/NIDDK NIH HHS/United States
- P01 DK68055/DK/NIDDK NIH HHS/United States
- U01 DK073985/DK/NIDDK NIH HHS/United States
- U01DK074007/DK/NIDDK NIH HHS/United States
- DK57061/DK/NIDDK NIH HHS/United States
- U01 DK073974/DK/NIDDK NIH HHS/United States
- P30 DK084567/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
