

Effect of mammography screening on surgical treatment for breast cancer in Norway: comparative analysis of cancer registry data
- PMID: 21914765
- PMCID: PMC3172323
- DOI: 10.1136/bmj.d4692
Effect of mammography screening on surgical treatment for breast cancer in Norway: comparative analysis of cancer registry data
Abstract
Objective: To determine the effect of mammography screening on surgical treatment for breast cancer.
Design: Comparative analysis of data from Norwegian cancer registry.
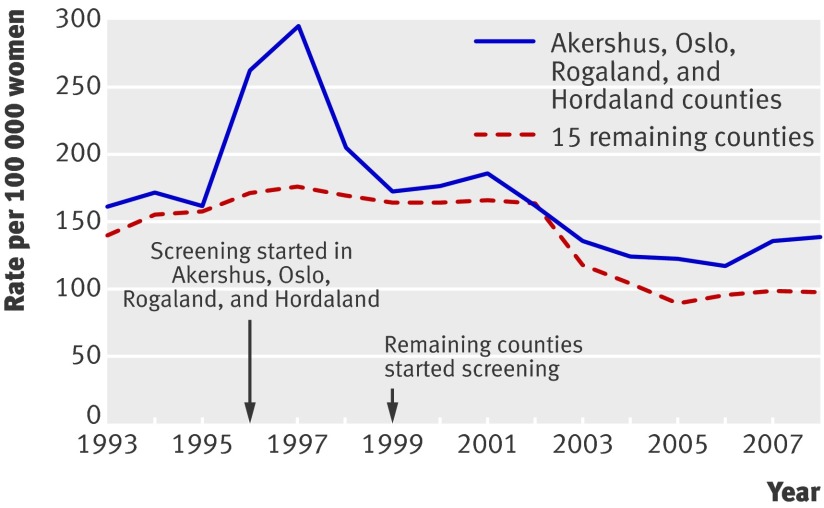
Setting: Mammography screening, Norway (screening of women aged 50-69 was introduced sequentially from 1996 to 2004).
Participants: 35,408 women aged 40-79 with invasive breast cancer or ductal carcinoma in situ treated surgically from 1993 to 2008.
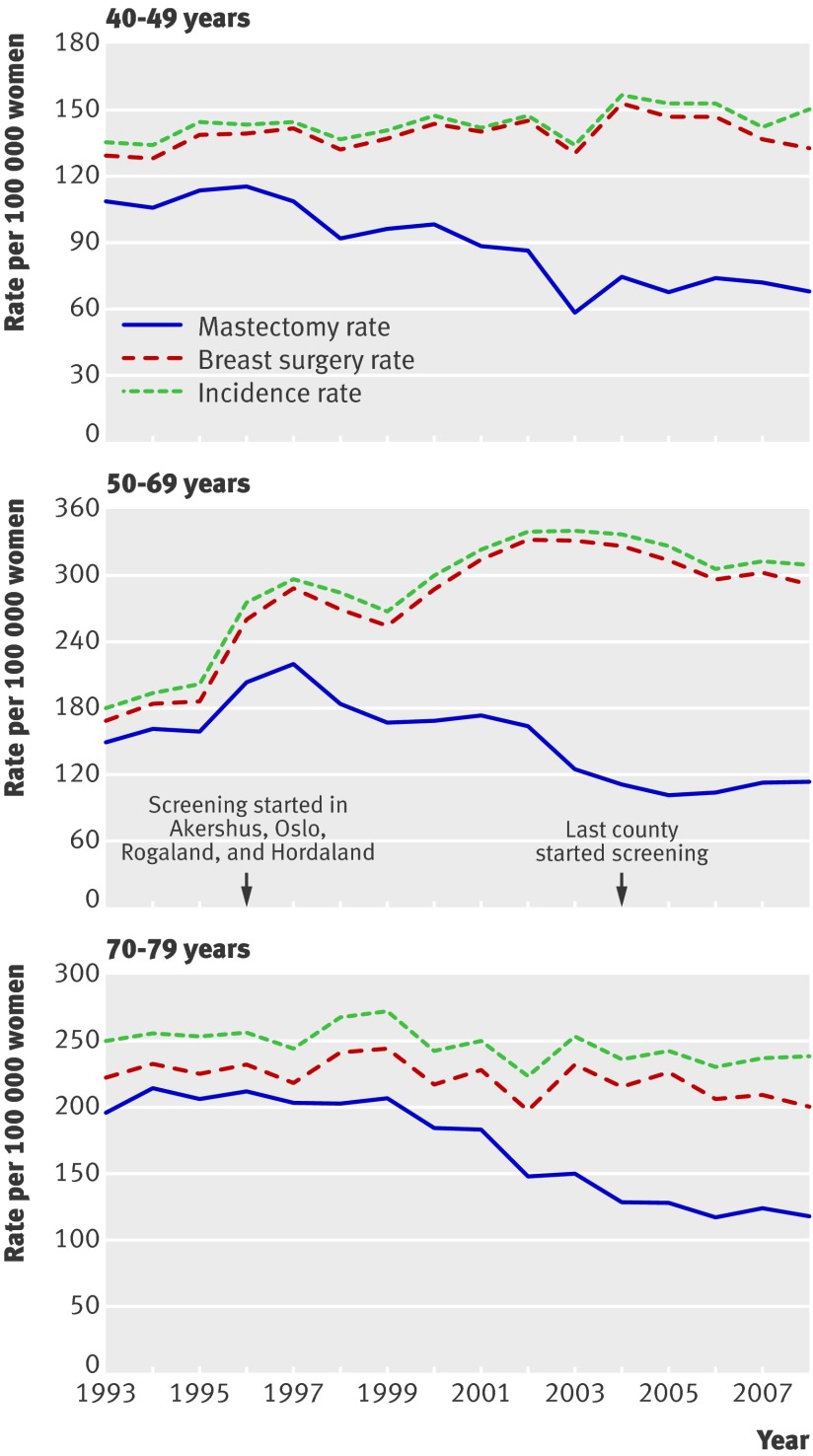
Main outcome measures: Rates of breast surgery (mastectomy plus breast conserving treatment) and rates of mastectomy for three age groups of women: 40-49, 50-69, and 70-79. Changes in rates from pre-screening period (1993-5) to introduction of screening phase (1996-2004) and then to screening period (2005-8) are presented as hazard ratios in invited and non-invited women.
Results: The annual rate for breast surgery from the pre-screening period (1993-5) to screening period (2005-8) in Norway increased by 70% (hazard ratio 1.70, 95% confidence interval 1.62 to 1.78), from 180 to 305 per 100,000 women in the invited age group (50-69 years). In the younger, non-invited age group (40-49 years), however, the increase was only 8% (1.08, 1.00 to 1.16), from 133 to 144 per 100,000 women per year, whereas in the older, non-invited age group (70-79 years) the rate decreased by 8% (0.92, 0.86 to 1.00), from 227 to 214 per 100,000 women per year. The rates for mastectomy decreased similarly from the pre-screening period to screening period in invited and non-invited women. From the pre-screening period to the introduction phase of screening (1996-2004), however, the annual mastectomy rate in women aged 50-69 invited to screening increased by 9% (1.09, 1.03 to 1.14), from 156 to 167 per 100,000 women, and in the younger non-invited women declined by 17% (0.83, 0.78 to 0.90), from 109 to 91 per 100,000 women. In consequence, the mastectomy rate was 31% (1.31, 1.20 to 1.43) higher in the invited than in the non-invited younger age group.
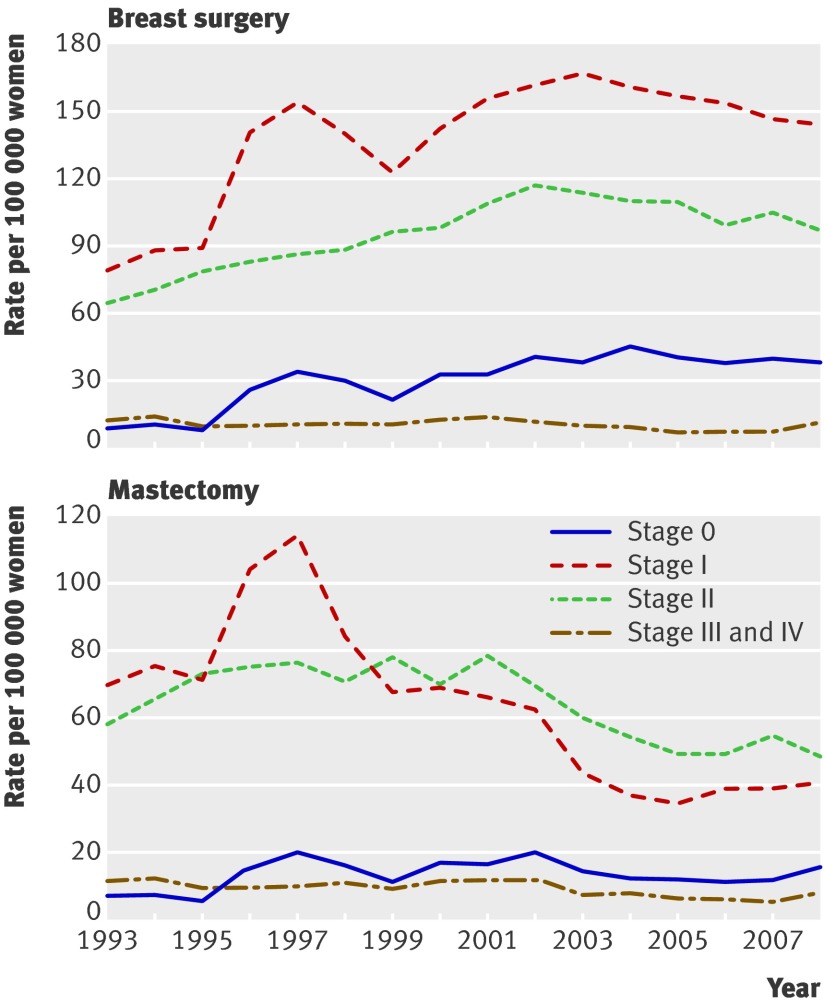
Conclusions: Mammography screening in Norway was associated with a noticeable increase in rates for breast cancer surgery in women aged 50-69 (the age group invited to screening) and also an increase in mastectomy rates. Although over-diagnosis is likely to have caused the initial increase in mastectomy rates and the overall increase in surgery rates in the age group screened, the more recent decline in mastectomy rates has affected all age groups and is likely to have resulted from changes in surgical policy.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Gøtzsche PC, Nielsen M. Screening for breast cancer with mammography. Cochrane Database Syst Rev 2009;CD001877. - PubMed
-
- Hofvind S, Geller B, Vacek PM, Thoresen S, Skaane P. Using the European guidelines to evaluate the Norwegian Breast Cancer Screening Program. Eur J Epidemiol 2007;22:447-55. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical