

Multicenter phase 2 trial of sirolimus for tuberous sclerosis: kidney angiomyolipomas and other tumors regress and VEGF- D levels decrease
- PMID: 21915260
- PMCID: PMC3167813
- DOI: 10.1371/journal.pone.0023379
Multicenter phase 2 trial of sirolimus for tuberous sclerosis: kidney angiomyolipomas and other tumors regress and VEGF- D levels decrease
Abstract
Background: Tuberous sclerosis (TSC) related tumors are characterized by constitutively activated mTOR signaling due to mutations in TSC1 or TSC2.
Methods: We completed a phase 2 multicenter trial to evaluate the efficacy and tolerability of the mTOR inhibitor, sirolimus, for the treatment of kidney angiomyolipomas.
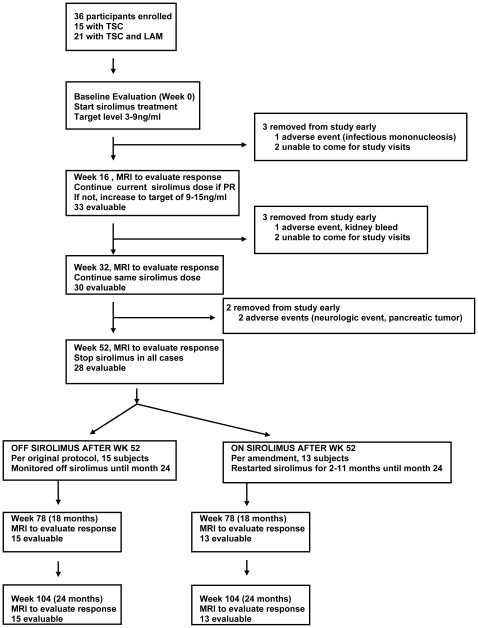
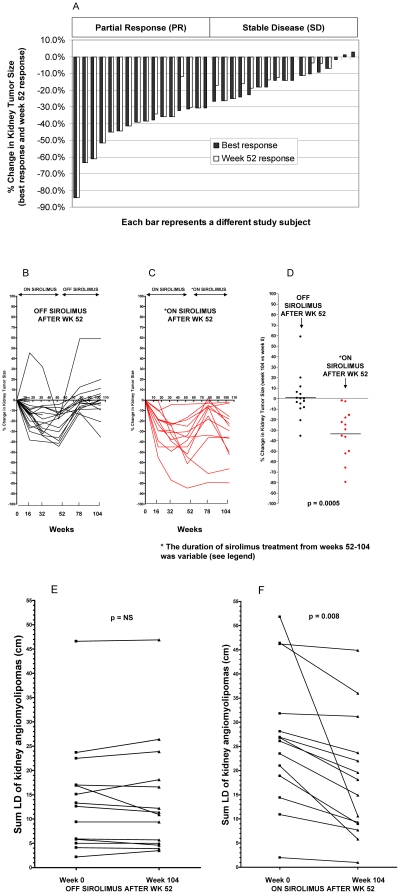
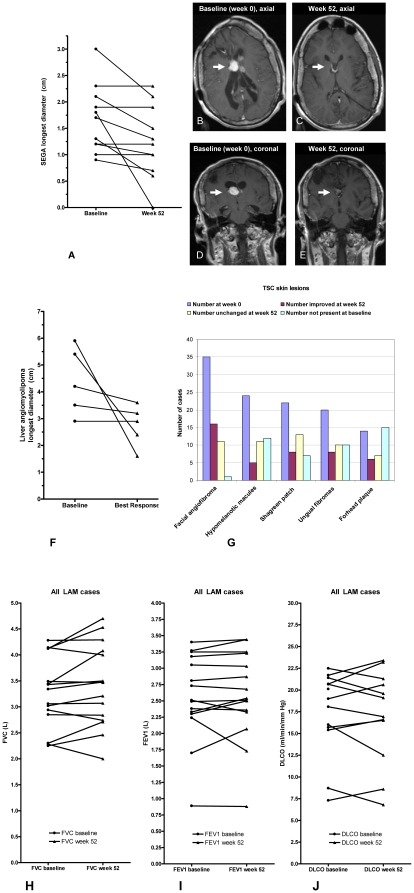
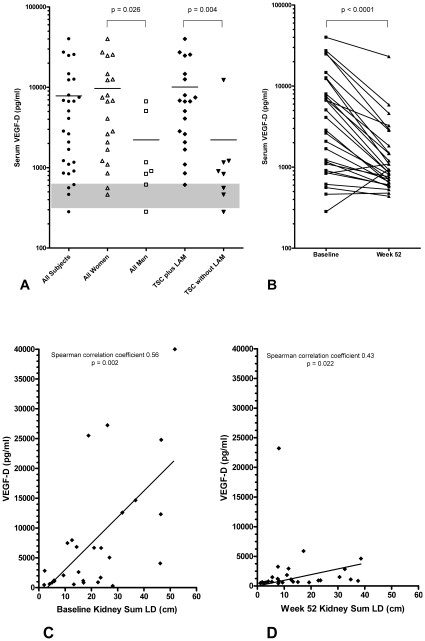
Results: 36 adults with TSC or TSC/LAM were enrolled and started on daily sirolimus. The overall response rate was 44.4% (95% confidence intervals [CI] 28 to 61); 16/36 had a partial response. The remainder had stable disease (47.2%, 17/36), or were unevaluable (8.3%, 3/36). The mean decrease in kidney tumor size (sum of the longest diameters [sum LD]) was 29.9% (95% CI, 22 to 37; n = 28 at week 52). Drug related grade 1-2 toxicities that occurred with a frequency of >20% included: stomatitis, hypertriglyceridemia, hypercholesterolemia, bone marrow suppression (anemia, mild neutropenia, leucopenia), proteinuria, and joint pain. There were three drug related grade 3 events: lymphopenia, headache, weight gain. Kidney angiomyolipomas regrew when sirolimus was discontinued but responses tended to persist if treatment was continued after week 52. We observed regression of brain tumors (SEGAs) in 7/11 cases (26% mean decrease in diameter), regression of liver angiomyolipomas in 4/5 cases (32.1% mean decrease in longest diameter), subjective improvement in facial angiofibromas in 57%, and stable lung function in women with TSC/LAM (n = 15). A correlative biomarker study showed that serum VEGF-D levels are elevated at baseline, decrease with sirolimus treatment, and correlate with kidney angiomyolipoma size (Spearman correlation coefficient 0.54, p = 0.001, at baseline).
Conclusions: Sirolimus treatment for 52 weeks induced regression of kidney angiomyolipomas, SEGAs, and liver angiomyolipomas. Serum VEGF-D may be a useful biomarker for monitoring kidney angiomyolipoma size. Future studies are needed to determine benefits and risks of longer duration treatment in adults and children with TSC.
Trial registration: Clinicaltrials.gov NCT00126672.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
