

Urine steroid metabolomics as a biomarker tool for detecting malignancy in adrenal tumors
- PMID: 21917861
- PMCID: PMC3232629
- DOI: 10.1210/jc.2011-1565
Urine steroid metabolomics as a biomarker tool for detecting malignancy in adrenal tumors
Abstract
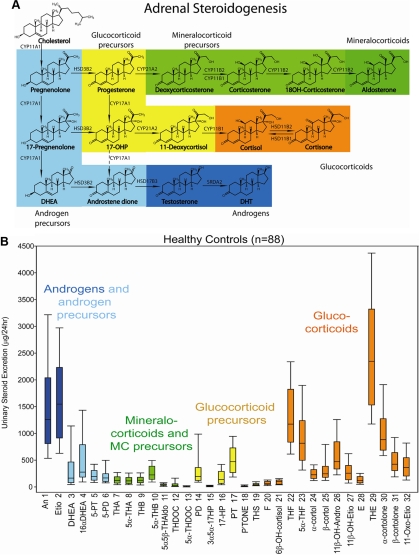
Context: Adrenal tumors have a prevalence of around 2% in the general population. Adrenocortical carcinoma (ACC) is rare but accounts for 2-11% of incidentally discovered adrenal masses. Differentiating ACC from adrenocortical adenoma (ACA) represents a diagnostic challenge in patients with adrenal incidentalomas, with tumor size, imaging, and even histology all providing unsatisfactory predictive values.
Objective: Here we developed a novel steroid metabolomic approach, mass spectrometry-based steroid profiling followed by machine learning analysis, and examined its diagnostic value for the detection of adrenal malignancy.
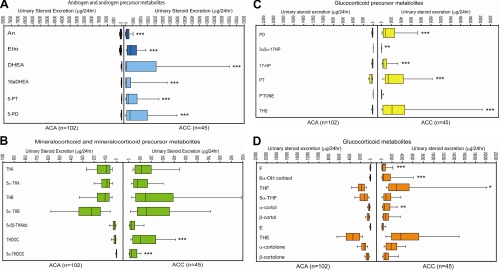
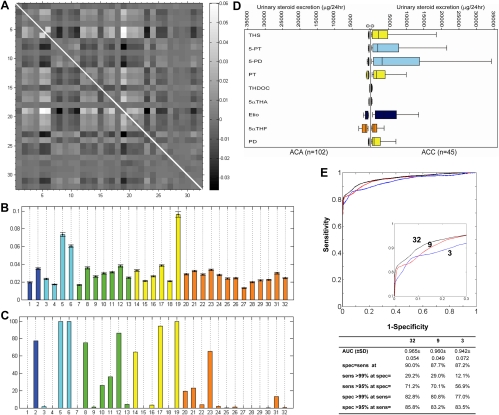
Design: Quantification of 32 distinct adrenal derived steroids was carried out by gas chromatography/mass spectrometry in 24-h urine samples from 102 ACA patients (age range 19-84 yr) and 45 ACC patients (20-80 yr). Underlying diagnosis was ascertained by histology and metastasis in ACC and by clinical follow-up [median duration 52 (range 26-201) months] without evidence of metastasis in ACA. Steroid excretion data were subjected to generalized matrix learning vector quantization (GMLVQ) to identify the most discriminative steroids.
Results: Steroid profiling revealed a pattern of predominantly immature, early-stage steroidogenesis in ACC. GMLVQ analysis identified a subset of nine steroids that performed best in differentiating ACA from ACC. Receiver-operating characteristics analysis of GMLVQ results demonstrated sensitivity = specificity = 90% (area under the curve = 0.97) employing all 32 steroids and sensitivity = specificity = 88% (area under the curve = 0.96) when using only the nine most differentiating markers.
Conclusions: Urine steroid metabolomics is a novel, highly sensitive, and specific biomarker tool for discriminating benign from malignant adrenal tumors, with obvious promise for the diagnostic work-up of patients with adrenal incidentalomas.
Figures
Comment in
-
A multi-test strategy for adrenal tumours.Lancet Diabetes Endocrinol. 2020 Sep;8(9):733-734. doi: 10.1016/S2213-8587(20)30224-2. Epub 2020 Jul 23. Lancet Diabetes Endocrinol. 2020. PMID: 32711726 No abstract available.
References
-
- Grumbach MM, Biller BM, Braunstein GD, Campbell KK, Carney JA, Godley PA, Harris EL, Lee JK, Oertel YC, Posner MC, Schlechte JA, Wieand HS. 2003. Management of the clinically inapparent adrenal mass (“incidentaloma”). Ann Intern Med 138:424–429 - PubMed
-
- Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR. 2004. The clinically inapparent adrenal mass: update in diagnosis and management. Endocr Rev 25:309–340 - PubMed
-
- Barzon L, Sonino N, Fallo F, Palu G, Boscaro M. 2003. Prevalence and natural history of adrenal incidentalomas. Eur J Endocrinol 149:273–285 - PubMed
-
- Terzolo M, Reimondo G, Angeli A. 2009. Definition of an optimal strategy to evaluate and follow-up adrenal incidentalomas: time for further research. Eur J Endocrinol 161:529–532 - PubMed
-
- Young WF., Jr 2007. Clinical practice. The incidentally discovered adrenal mass. N Engl J Med 356:601–610 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
