

Abacavir/lamivudine versus tenofovir DF/emtricitabine as part of combination regimens for initial treatment of HIV: final results
- PMID: 21917892
- PMCID: PMC3173503
- DOI: 10.1093/infdis/jir505
Abacavir/lamivudine versus tenofovir DF/emtricitabine as part of combination regimens for initial treatment of HIV: final results
Abstract
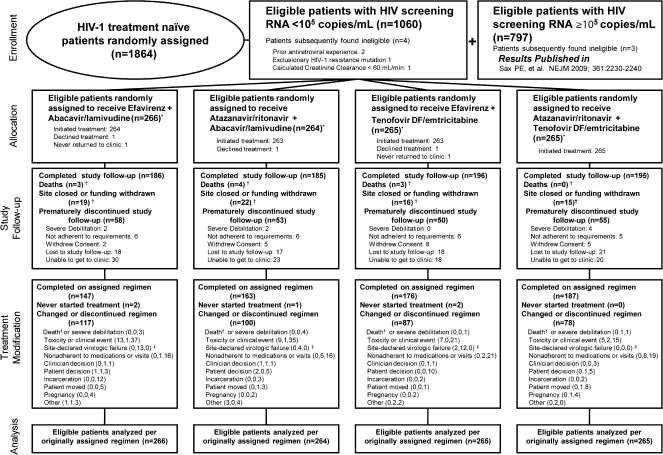
Background: AIDS Clinical Trials Group A5202 compared blinded abacavir/lamivudine (ABC/3TC) to tenofovir DF/emtricitabine (TDF/FTC) with efavirenz (EFV) or atazanavir/ritonavir (ATV/r) in human immunodeficiency virus (HIV)-infected treatment-naive patients, stratified by screening HIV RNA (< or ≥ 10(5) copies/mL). Due to higher virologic failure with ABC/3TC in the high HIV RNA stratum, blinded treatment was stopped in this group, but study follow-up continued for all patients.
Methods: Primary endpoints were times to virologic failure, regimen modification, and safety event.
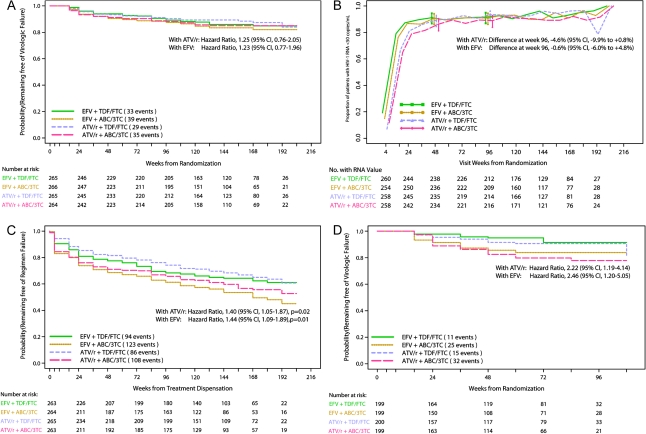
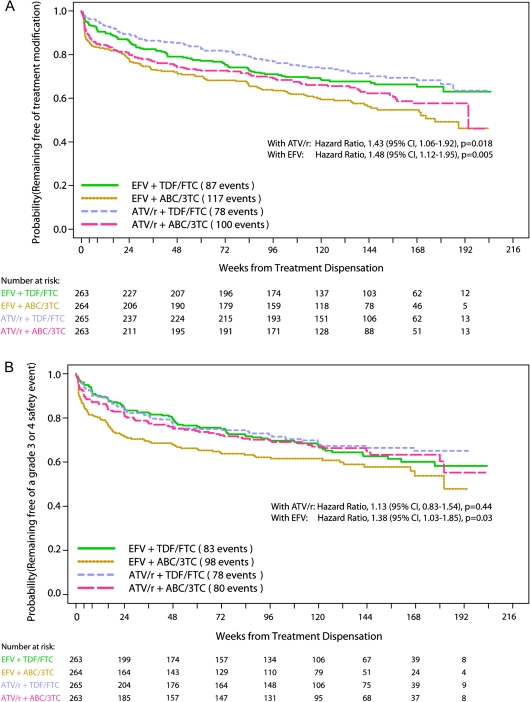
Results: In the low HIV RNA stratum, time to virologic failure was similar for ABC/3TC vs TDF/FTC with ATV/r (hazard ratio [HR] 1.25, 95% confidence interval [CI] 0.76, 2.05) or EFV (HR 1.23, 95% CI 0.77, 1.96), with significantly shorter times to regimen modification for ABC/3TC with EFV or ATV/r and to safety events with EFV. Prior to stopping blinded treatment in the high stratum, higher virologic failure rates were seen with ABC/3TC with EFV (HR 2.46, 95% CI 1.20, 5.05) or ATV/r (HR 2.22, 95% CI 1.19, 4.14).
Conclusions: In the low HIV RNA stratum, times to virologic failure for ABC/3TC or TDF/FTC were not different with EFV or ATV/r. In the high stratum, virologic failure rate was significantly higher for ABC/3TC than for TDF/FTC when given with either EFV or ATV/r.
Figures
Comment in
-
Optimizing initial therapy for HIV infection.J Infect Dis. 2011 Oct 15;204(8):1154-6. doi: 10.1093/infdis/jir506. J Infect Dis. 2011. PMID: 21917886 Free PMC article. No abstract available.
References
-
- Thompson MA, Aberg JA, Cahn P, et al. Antiretroviral treatment of adult HIV infection: 2010 recommendations of the International AIDS Society-USA panel. JAMA. 2010;304:321–33. - PubMed
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services; 2011. pp. 1–174. http://aidsinfo.nih.gov/contentfiles/AdultandAdolescentGL.pdf. Accessed 28 August 2011.
-
- DeJesus E, Herrera G, Teofilo E, et al. Abacavir versus zidovudine combined with lamivudine and efavirenz, for the treatment of antiretroviral-naive HIV-infected adults. Clin Infect Dis. 2004;39:1038–46. Epub 2004. - PubMed
-
- Gallant JE, DeJesus E, Arribas JR, et al. Tenofovir DF, emtricitabine, and efavirenz vs. zidovudine, lamivudine, and efavirenz for HIV. N Engl J Med. 2006;354:251–60. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 AI046376/AI/NIAID NIH HHS/United States
- 1U01 AI069494-01/AI/NIAID NIH HHS/United States
- U01 AI069477/AI/NIAID NIH HHS/United States
- U01 AI069502/AI/NIAID NIH HHS/United States
- M01-RR00425/RR/NCRR NIH HHS/United States
- U01 AI069513/AI/NIAID NIH HHS/United States
- AI68634/AI/NIAID NIH HHS/United States
- UM1 AI069423/AI/NIAID NIH HHS/United States
- UL1 RR033176/RR/NCRR NIH HHS/United States
- U01 AI069474/AI/NIAID NIH HHS/United States
- U01 AI069434/AI/NIAID NIH HHS/United States
- AI69556/AI/NIAID NIH HHS/United States
- U01 AI069447/AI/NIAID NIH HHS/United States
- UM1 AI069501/AI/NIAID NIH HHS/United States
- UM1 AI069472/AI/NIAID NIH HHS/United States
- U01 AI069467/AI/NIAID NIH HHS/United States
- P30 AI050409/AI/NIAID NIH HHS/United States
- U01 AI069423/AI/NIAID NIH HHS/United States
- UM1 AI069513/AI/NIAID NIH HHS/United States
- 5U01 AI069484-02/AI/NIAID NIH HHS/United States
- AI58740/AI/NIAID NIH HHS/United States
- 5U01 AI069415-03/AI/NIAID NIH HHS/United States
- M01 RR000046/RR/NCRR NIH HHS/United States
- AI69419/AI/NIAID NIH HHS/United States
- 1U01 AI069472-01/AI/NIAID NIH HHS/United States
- AI46370/AI/NIAID NIH HHS/United States
- AI032782/AI/NIAID NIH HHS/United States
- U01 AI027661/AI/NIAID NIH HHS/United States
- UM1 AI069424/AI/NIAID NIH HHS/United States
- AI25868/AI/NIAID NIH HHS/United States
- AI69501/AI/NIAID NIH HHS/United States
- AI27675/AI/NIAID NIH HHS/United States
- U01 AI069465/AI/NIAID NIH HHS/United States
- UM1 AI069434/AI/NIAID NIH HHS/United States
- 5P30 AI045008-10/AI/NIAID NIH HHS/United States
- UL1 RR024996/RR/NCRR NIH HHS/United States
- AI27666/AI/NIAID NIH HHS/United States
- UM1 AI069432/AI/NIAID NIH HHS/United States
- AI069501/AI/NIAID NIH HHS/United States
- 5U01 AI069428/AI/NIAID NIH HHS/United States
- U54 RR023561/RR/NCRR NIH HHS/United States
- UL1 RR025780/RR/NCRR NIH HHS/United States
- AI069532/AI/NIAID NIH HHS/United States
- AI069474/AI/NIAID NIH HHS/United States
- AI069434/AI/NIAID NIH HHS/United States
- U01 AI069470/AI/NIAID NIH HHS/United States
- UM1 AI069495/AI/NIAID NIH HHS/United States
- AI38858/AI/NIAID NIH HHS/United States
- U01 AI069484/AI/NIAID NIH HHS/United States
- AI69423/AI/NIAID NIH HHS/United States
- UM1 AI069471/AI/NIAID NIH HHS/United States
- U01 AI069439/AI/NIAID NIH HHS/United States
- U01 AI069556/AI/NIAID NIH HHS/United States
- U0I A106947203/PHS HHS/United States
- UL1 RR024156/RR/NCRR NIH HHS/United States
- U01 AI069418/AI/NIAID NIH HHS/United States
- AI069513/AI/NIAID NIH HHS/United States
- U01 AI069428/AI/NIAID NIH HHS/United States
- U01 AI069467-03/AI/NIAID NIH HHS/United States
- 1UL1 RR024156/RR/NCRR NIH HHS/United States
- U01 AI069532/AI/NIAID NIH HHS/United States
- UM1 AI069439/AI/NIAID NIH HHS/United States
- U01 AI069452-03/AI/NIAID NIH HHS/United States
- UL1 TR000124/TR/NCATS NIH HHS/United States
- 1UL1 RR025777-01/RR/NCRR NIH HHS/United States
- UM1 AI069415/AI/NIAID NIH HHS/United States
- 5U01 AI069471/AI/NIAID NIH HHS/United States
- AI27661/AI/NIAID NIH HHS/United States
- AI069439/AI/NIAID NIH HHS/United States
- P30 AI045008/AI/NIAID NIH HHS/United States
- 5U01 A1027658/PHS HHS/United States
- AI34853/AI/NIAID NIH HHS/United States
- 1U01 AI069502-01/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- U01 AI069501/AI/NIAID NIH HHS/United States
- R01 AI058740/AI/NIAID NIH HHS/United States
- AI069495/AI/NIAID NIH HHS/United States
- 5U01 AI069418/AI/NIAID NIH HHS/United States
- UM1 AI069477/AI/NIAID NIH HHS/United States
- U01 AI069432/AI/NIAID NIH HHS/United States
- AI073961/AI/NIAID NIH HHS/United States
- U01 AI046370/AI/NIAID NIH HHS/United States
- U01 AI068636/AI/NIAID NIH HHS/United States
- U01 AI038858/AI/NIAID NIH HHS/United States
- 5U01 AI069447 03/AI/NIAID NIH HHS/United States
- P30 AI073961/AI/NIAID NIH HHS/United States
- UM1 AI069474/AI/NIAID NIH HHS/United States
- AI69465/AI/NIAID NIH HHS/United States
- UL1 RR025777/RR/NCRR NIH HHS/United States
- U01 AI034853/AI/NIAID NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- AI069424/AI/NIAID NIH HHS/United States
- U01 AI069415/AI/NIAID NIH HHS/United States
- U01 AI027666/AI/NIAID NIH HHS/United States
- UL1 RR024160/RR/NCRR NIH HHS/United States
- 5U01 AI069470/AI/NIAID NIH HHS/United States
- U01 AI069495/AI/NIAID NIH HHS/United States
- 1U01 AI69467-01/AI/NIAID NIH HHS/United States
- UM1 AI069556/AI/NIAID NIH HHS/United States
- U01 AI027675/AI/NIAID NIH HHS/United States
- M01 RR000425/RR/NCRR NIH HHS/United States
- U01 AI069511/AI/NIAID NIH HHS/United States
- RR025747/RR/NCRR NIH HHS/United States
- U01 AI025859/AI/NIAID NIH HHS/United States
- UL1 RR025747/RR/NCRR NIH HHS/United States
- UM1 AI069532/AI/NIAID NIH HHS/United States
- UM1 AI069465/AI/NIAID NIH HHS/United States
- U01 AI069424/AI/NIAID NIH HHS/United States
- 3U01 AI046376 05S4/AI/NIAID NIH HHS/United States
- U01 AI032782/AI/NIAID NIH HHS/United States
- 1U01 A1069423-01/PHS HHS/United States
- AI069472/AI/NIAID NIH HHS/United States
- UM1 AI069419/AI/NIAID NIH HHS/United States
- RR025780/RR/NCRR NIH HHS/United States
- 5U01 AI069470-03/AI/NIAID NIH HHS/United States
- N01 AI72626/AI/NIAID NIH HHS/United States
- AI50410/AI/NIAID NIH HHS/United States
- U01 AI069419/AI/NIAID NIH HHS/United States
- U01 AI069494/AI/NIAID NIH HHS/United States
- U01AI068636/AI/NIAID NIH HHS/United States
- AI69432/AI/NIAID NIH HHS/United States
- U01 AI069452/AI/NIAID NIH HHS/United States
- AI069477/AI/NIAID NIH HHS/United States
- RR024996/RR/NCRR NIH HHS/United States
- RR00046/RR/NCRR NIH HHS/United States
- AI069471/AI/NIAID NIH HHS/United States
- U01 AI069471/AI/NIAID NIH HHS/United States
- U01 AI069472/AI/NIAID NIH HHS/United States
- U01 AI068634/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- U01 AI025868/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
