

Immunologic failure despite suppressive antiretroviral therapy is related to activation and turnover of memory CD4 cells
- PMID: 21917895
- PMCID: PMC3218674
- DOI: 10.1093/infdis/jir507
Immunologic failure despite suppressive antiretroviral therapy is related to activation and turnover of memory CD4 cells
Abstract
Background: Failure to normalize CD4(+) T-cell numbers despite effective antiretroviral therapy is an important problem in human immunodeficiency virus (HIV) infection.
Methods: To evaluate potential determinants of immune failure in this setting, we performed a comprehensive immunophenotypic characterization of patients with immune failure despite HIV suppression, persons who experienced CD4(+) T-cell restoration with therapy, and healthy controls.
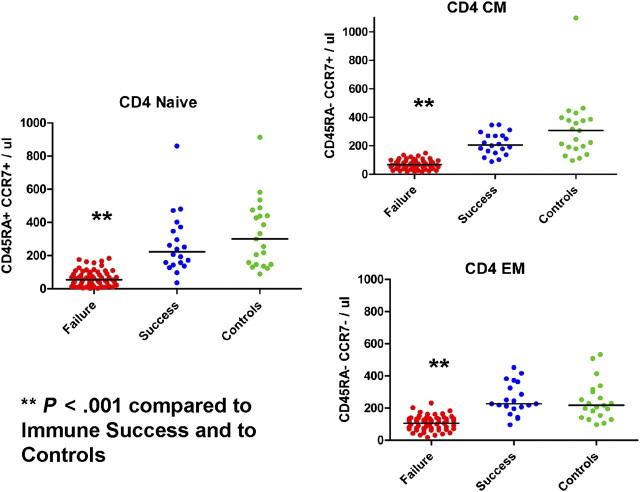
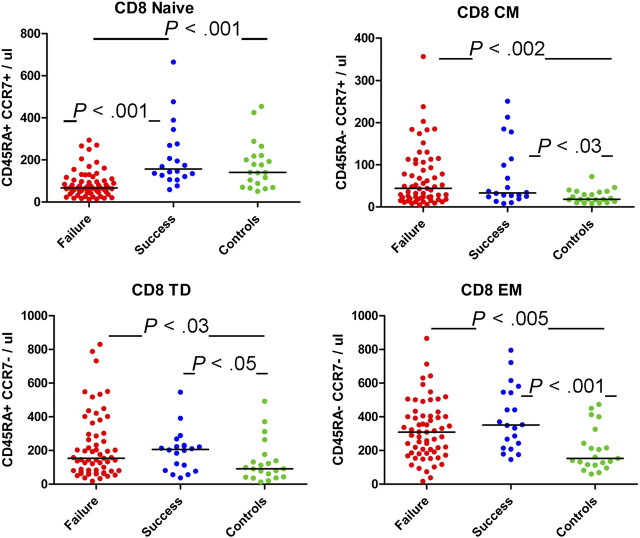
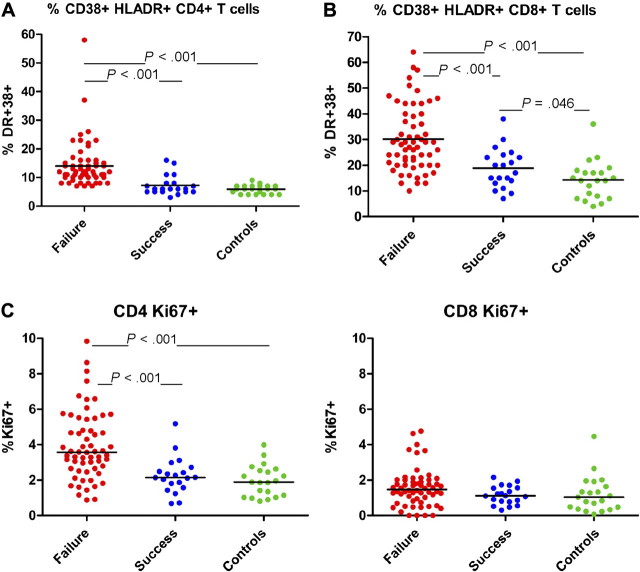
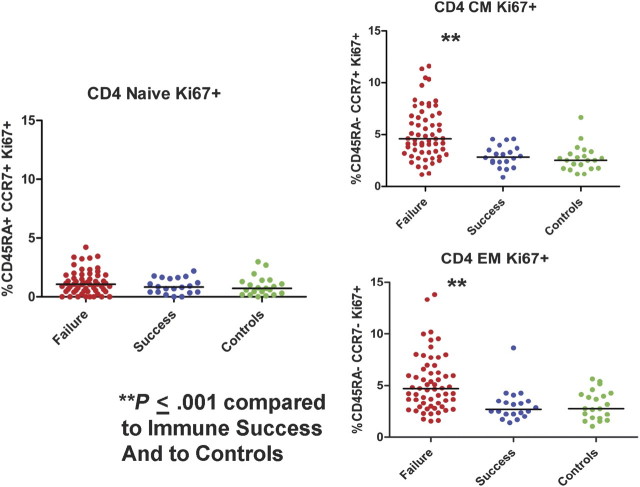
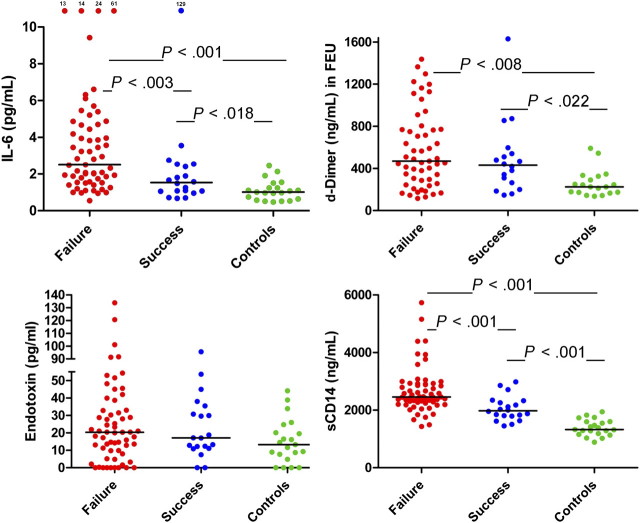
Results: Profound depletion of all CD4(+) T-cell maturation subsets and depletion of naive CD8(+) T cells was found in immune failure, implying failure of T-cell production/expansion. In immune failure, both CD4(+) and CD8(+) cells were activated but only memory CD4(+) cells were cycling at increased frequency. This may be the consequence of inflammation induced by in vivo exposure to microbial products, as soluble levels of the endotoxin receptor CD14(+) and interleukin 6 were elevated in immune failure. In multivariate analyses, naive T-cell depletion, phenotypic activation (CD38(+) and HLA-DR expression), cycling of memory CD4(+) T cells, and levels of soluble CD14 (sCD14) distinguished immune failure from immune success, even when adjusted for CD4(+) T-cell nadir, age at treatment initiation, and other clinical indices.
Conclusions: Immune activation that appears related to exposure to microbial elements distinguishes immune failure from immune success in treated HIV infection.
Figures
References
-
- Palella FJ, Jr, Baker RK, Moorman AC, et al. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr. 2006;43:27–34. - PubMed
-
- Keiser O, Taffe P, Zwahlen M, et al. All cause mortality in the Swiss HIV Cohort Study from 1990 to 2001 in comparison with the Swiss population. AIDS. 2004;18:1835–43. - PubMed
-
- Lewden C, Chene G, Morlat P, et al. HIV-infected adults with a CD4 cell count greater than 500 cells/mm3 on long-term combination antiretroviral therapy reach same mortality rates as the general population. J Acquir Immune Defic Syndr. 2007;46:72–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
