

Bony impingement limits design-related increases in hip range of motion
- PMID: 21918798
- PMCID: PMC3254736
- DOI: 10.1007/s11999-011-2096-3
Bony impingement limits design-related increases in hip range of motion
Abstract
Background: Factors affecting risk for impingement and dislocation can be related to the patient, implant design, or surgeon. While these have been studied independently, the impact of each factor relative to the others is not known.
Questions/purposes: We determined the effect of three implant design factors, prosthetic placement, and patient anatomy on subject-specific ROM.
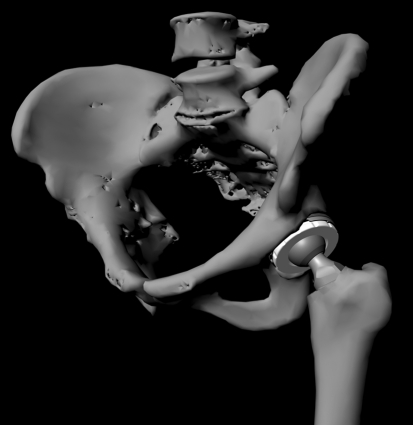
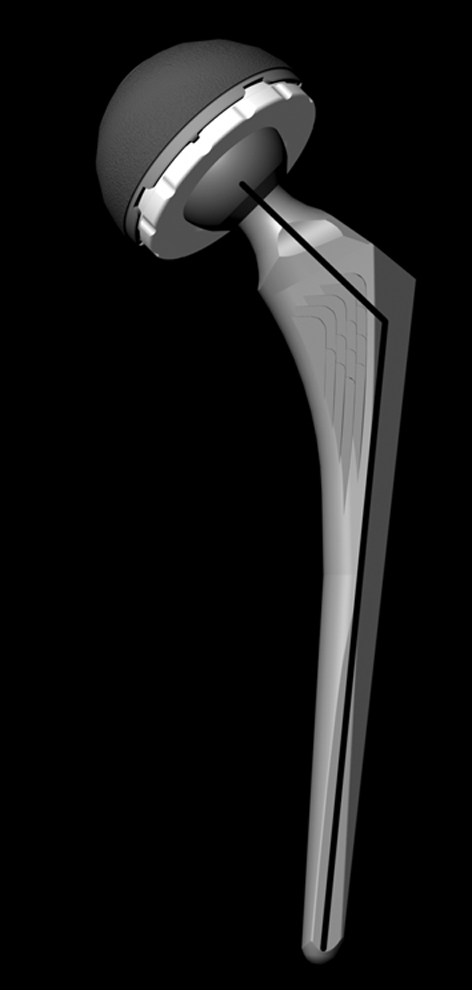
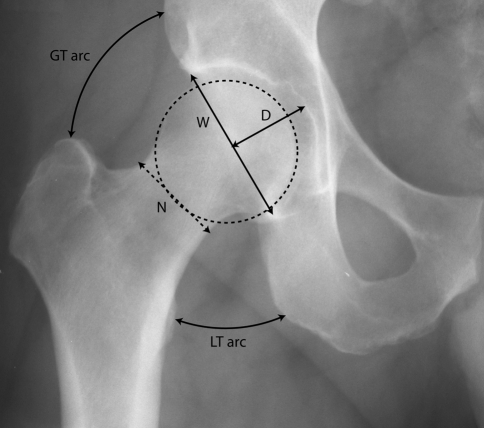
Methods: We virtually implanted hip geometry obtained from 16 CT scans using computer models of hip components with differences in head size, neck diameter, and neck-shaft angle. A contact detection model computed ROM before prosthetic or bony impingement. We correlated anatomic measurements from pelvic radiographs with ROM.
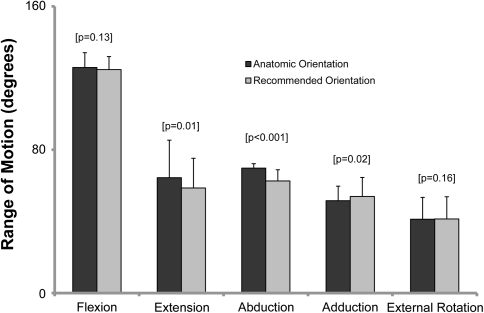
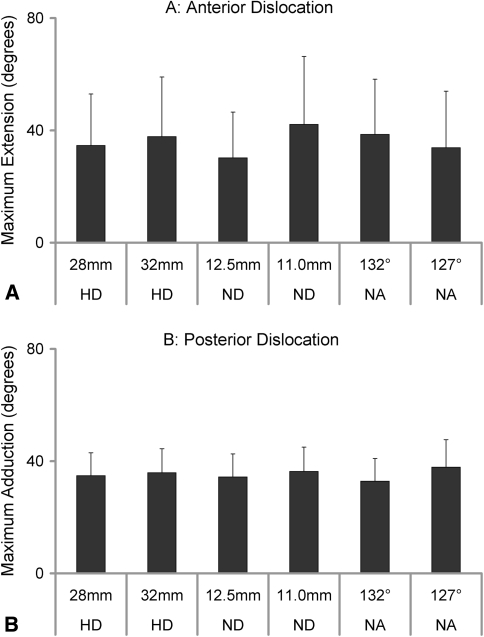
Results: When we implanted the components for best fit to the subject's anatomy or in the recommended orientation of 45° abduction and 20° anteversion, ROM was greater than 110° of flexion, 30° of extension, 45° of adduction-abduction, and 40° of external rotation. Changes in head size, neck diameter, and neck-shaft angle generated small gains (3.6°-6°) in ROM when analyzed individually, but collectively, we noted a more substantial increase (10°-17°). Radiographic measurements correlated only moderately with hip flexion and abduction.
Conclusions: It is feasible to tailor implant placement to each patient to maximize bony coverage without compromising ROM. Once bony impingement becomes the restricting factor, further changes in implant design may not improve ROM. Radiographic measurements do not appear to have value in predicting ROM.
Figures

References
-
- Bartz RL, Nobel PC, Kadakia NR, Tullos HS. The effect of femoral component head size on posterior dislocation of the artificial hip joint. J Bone Joint Surg Am. 2000;82:1300–1307. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
