

Reducing patient radiation dose during CT-guided procedures: demonstration in spinal injections for pain
- PMID: 21920858
- PMCID: PMC7966006
- DOI: 10.3174/ajnr.A2634
Reducing patient radiation dose during CT-guided procedures: demonstration in spinal injections for pain
Abstract
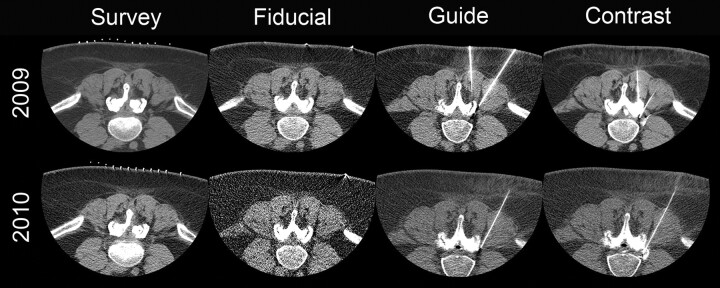
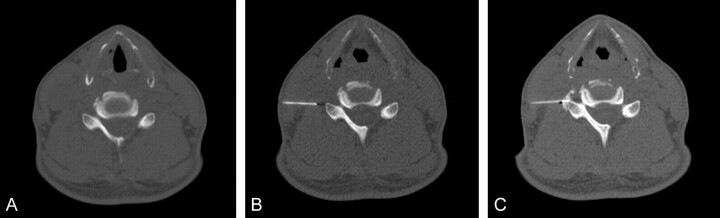
Background and purpose: CT guidance may improve precision for diagnostic and therapeutic spinal injections, but it can increase patient radiation dose. This study examined the impact of reducing tube current on patient radiation exposure and the technical success for these procedures, by using axial acquisitions for short scan lengths and eliminating nonessential imaging.
Materials and methods: Our institutional review board approved retrospective analysis of records from 100 consecutive outpatients undergoing spinal injections for pain before and after the CT protocol modification to reduce radiation dose. Data collected included patient age and sex, response to injection, number of sites and spinal levels treated, injection type, performing physician, CT acquisition method, number of imaging series, tube current, scan length, and DLP.
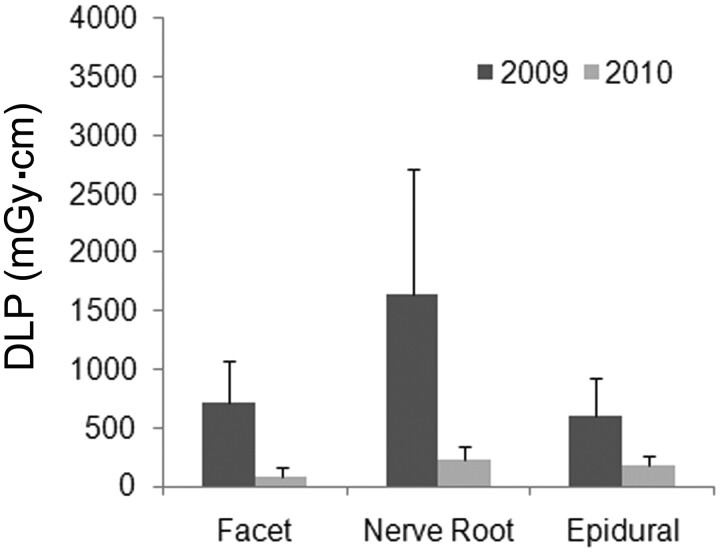
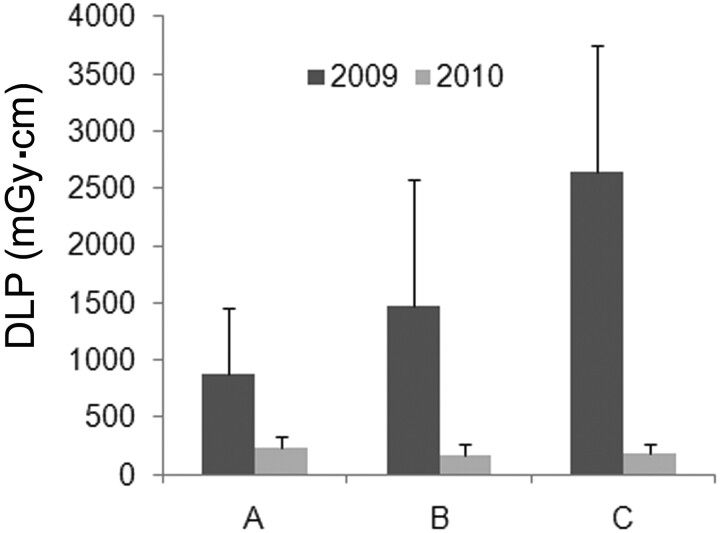
Results: Image contrast was reduced with the low-dose protocol, but this did not affect technical success or immediate pain relief. Mean DLP for all procedures decreased from 1458 ± 1022 to 199 ± 101 mGy · cm (P < .001). The range of radiologist-dependent DLP per procedure also was reduced significantly with the modified protocol. Selective nerve root blocks, lumbar injections, multiple injection sites, and the lack of prior imaging were each associated with a slightly higher DLP (<50 mGy · cm).
Conclusions: Radiation to patients undergoing CT-guided spinal injections can be decreased significantly without affecting outcome by reducing tube current, using axial acquisitions for short scan lengths, and eliminating nonessential imaging guidance. These measures also decrease variability in radiation doses between different practitioners and should be useful for other CT-guided procedures in radiology.
Figures



References
-
- Gangi A, Dietemann JL, Mortazavi R, et al. . CT-guided interventional procedures for pain management in the lumbosacral spine. Radiographics 1998;18:621–33 - PubMed
-
- Deyo RA, Weinstein JN.. Low back pain. N Engl J Med 2001;344:363–70 - PubMed
-
- Brenner DJ, Hall EJ.. Computed tomography: an increasing source of radiation exposure. N Engl J Med 2007;357:2277–84 - PubMed
-
- Bogdanich W.. Radiation overdoses point up dangers of CT scans. New York Times. October 16, 2009;A13
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical