

Detection of intracochlear damage with cochlear implantation in a gerbil model of hearing loss
- PMID: 21921858
- PMCID: PMC3338854
- DOI: 10.1097/MAO.0b013e31822f09f2
Detection of intracochlear damage with cochlear implantation in a gerbil model of hearing loss
Abstract
Hypothesis: Cochlear trauma due to electrode insertion can be detected in acoustic responses to low frequencies in an animal model with a hearing condition similar to patients using electroacoustic stimulation.
Background: Clinical evidence suggests that intracochlear damage during cochlear implantation negatively affects residual hearing. Recently, we demonstrated the usefulness of acoustically evoked potentials to detect cochlear trauma in normal-hearing gerbils. Here, gerbils with noise-induced hearing loss were used to investigate the effects of remote trauma on residual hearing.
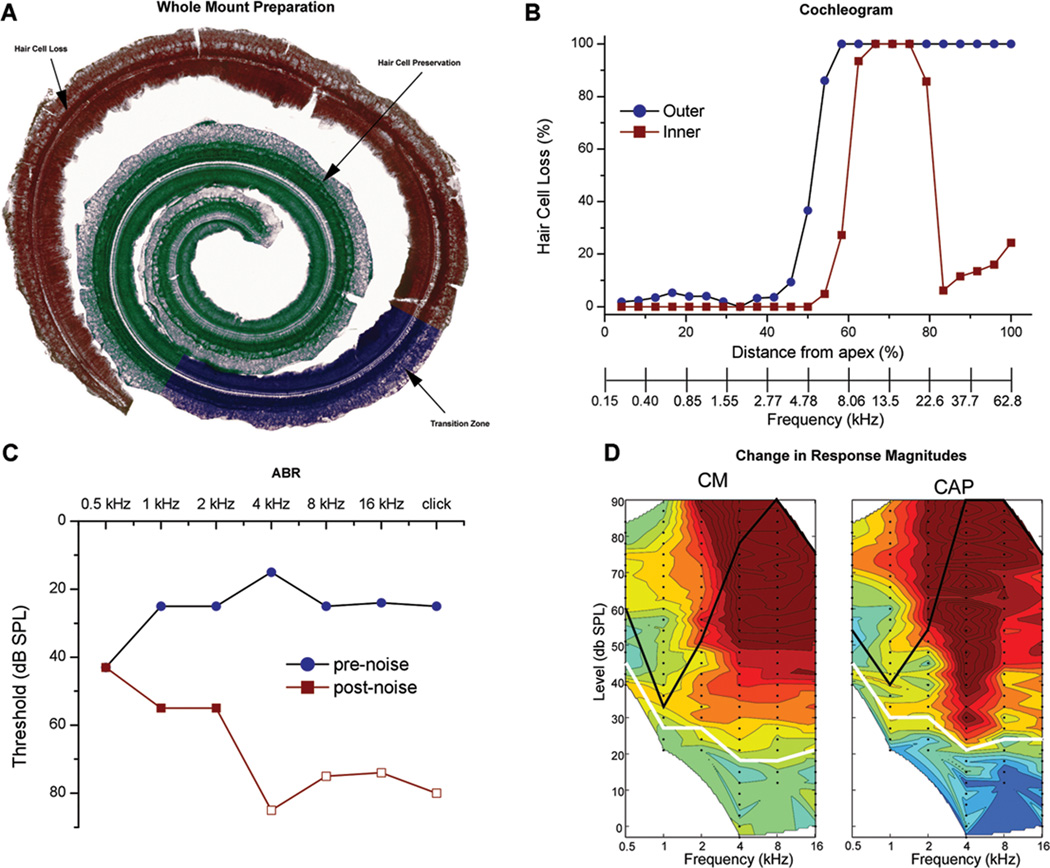
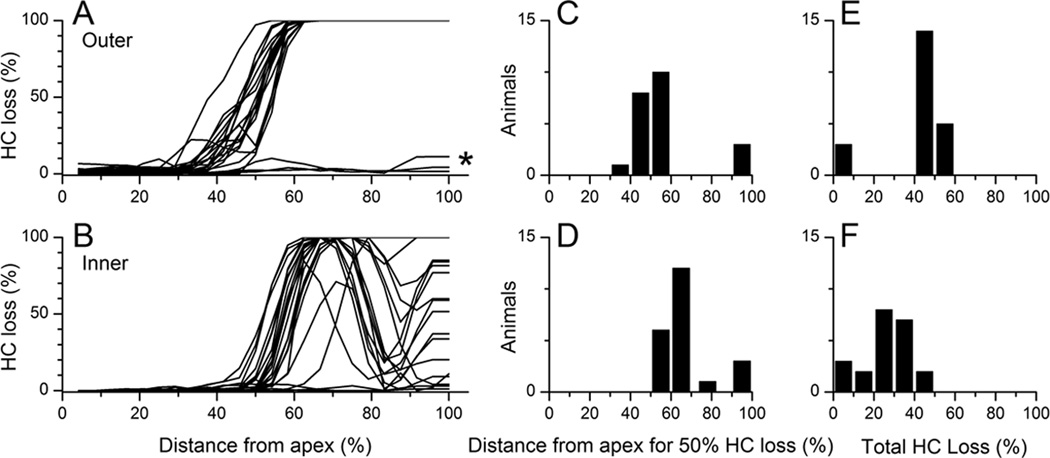
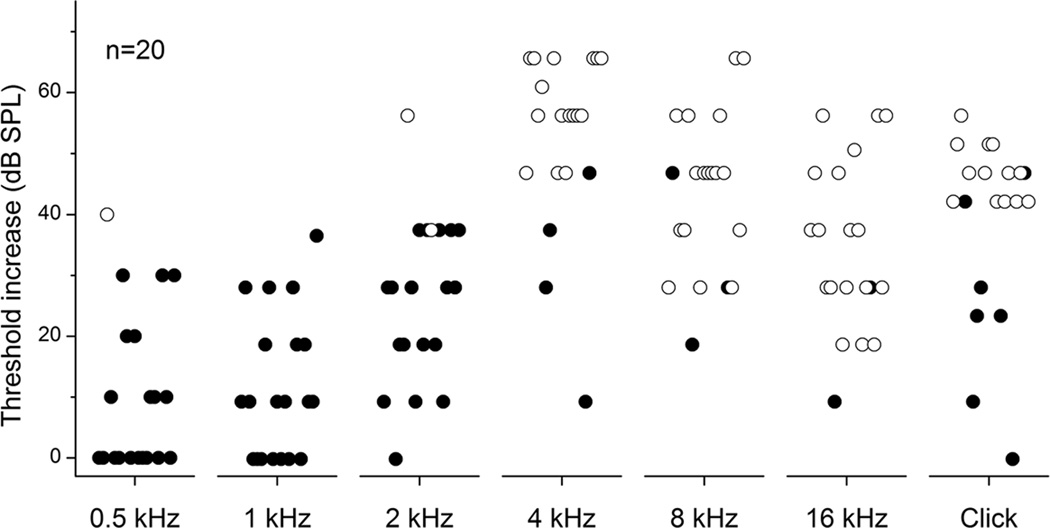
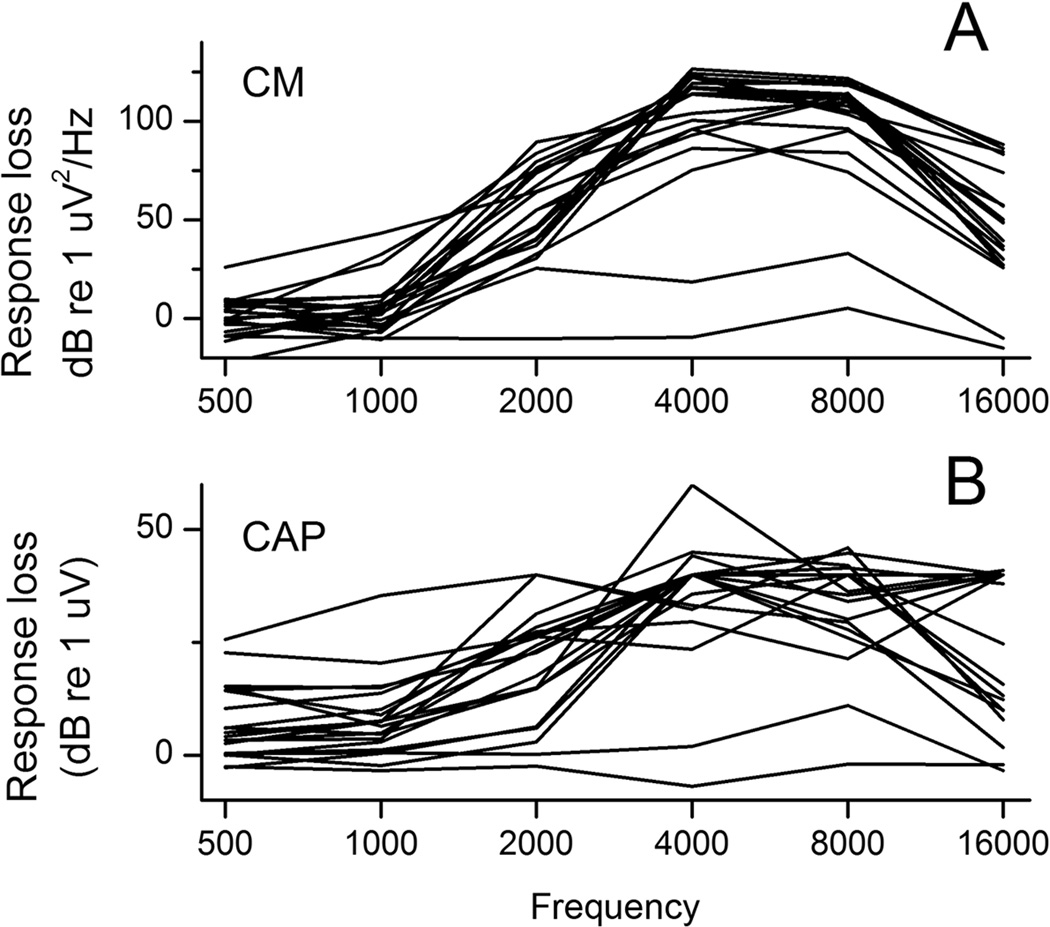
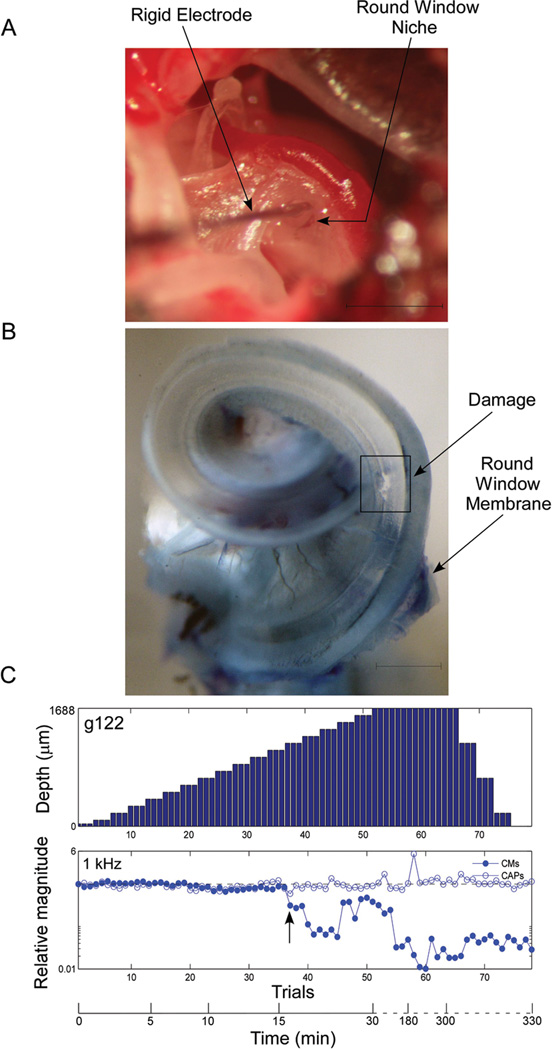
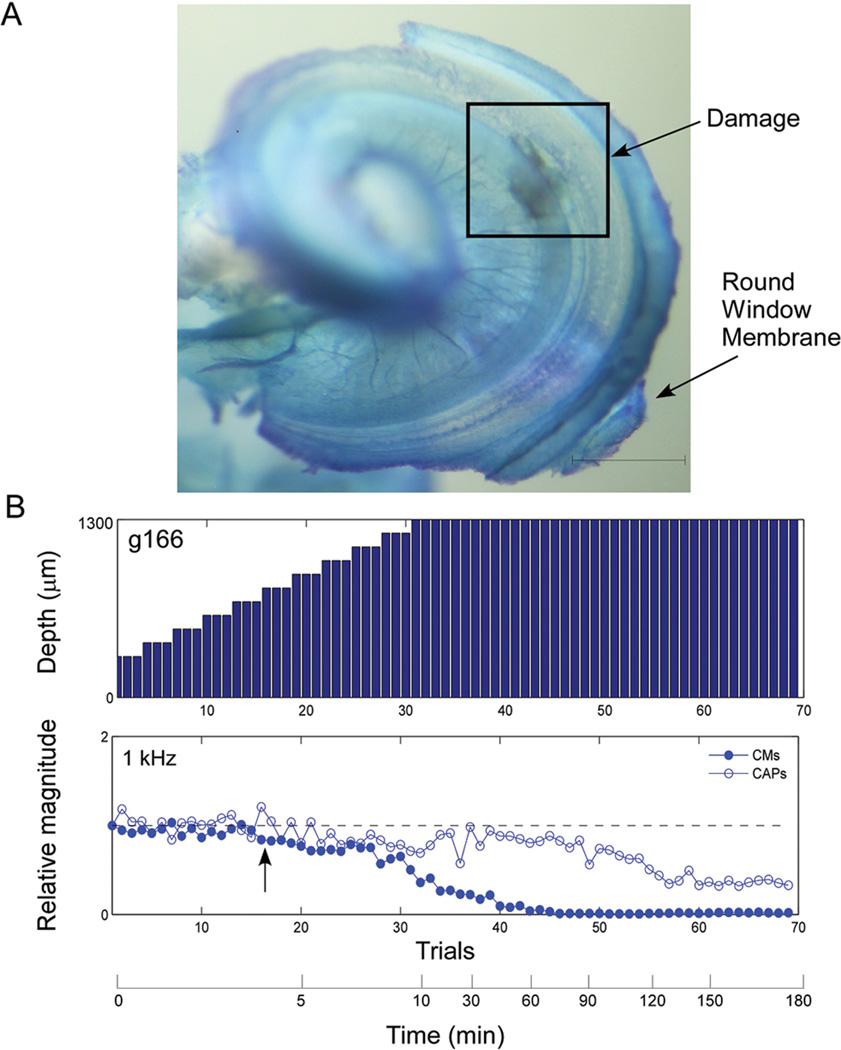
Methods: Gerbils underwent high-pass (4-kHz cutoff) noise exposure to produce sloping hearing loss. After 1 month of recovery, each animal's hearing loss was determined from auditory brainstem responses and baseline intracochlear recording of the cochlear microphonic and compound action potential (CAP) obtained at the round window. Subsequently, electrode insertions were performed to produce basal trauma, whereas the acoustically generated potentials to a 1-kHz tone-burst were recorded after each step of electrode advancement. Hair cell counts were made to characterize the noise damage, and cochlear whole mounts were used to identify cochlear trauma due to the electrode.
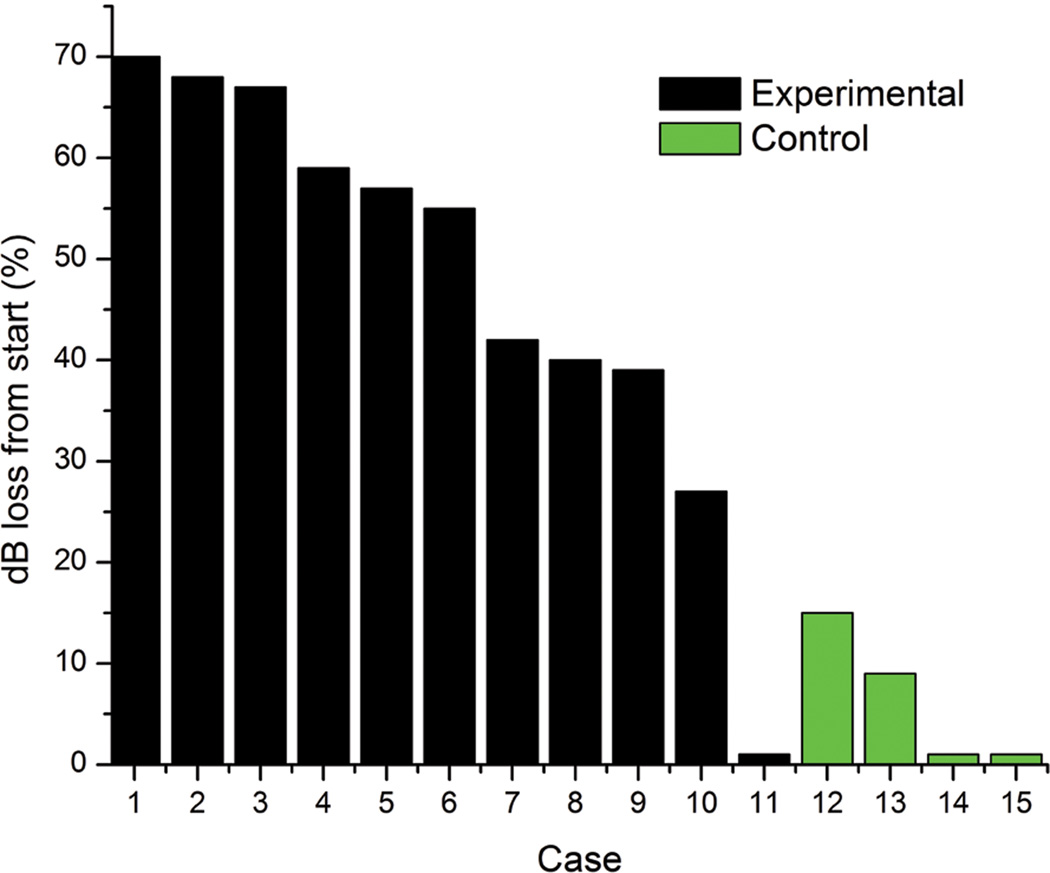
Results: The noise exposure paradigm produced a pattern of hair cell, auditory brainstem response, and intracochlear potential losses that closely mimicked that of electrical and acoustic stimulation patients. Trauma in the basal turn, in the 15- to 30-kHz portion of the deafened region, remote from preserved hair cells, induced a decline in intracochlear acoustic responses to the hearing preserved frequency of 1 kHz.
Conclusion: The results indicate that a recording algorithm based on physiological markers to low-frequency acoustic stimuli can identify cochlear trauma during implantation. Future work will focus on translating these results for use with current cochlear implant technology in humans.
Conflict of interest statement
Figures
References
-
- Cullen RD, Higgins C, Buss E, Clark M, Pillsbury HC, 3rd, Buchman CA. Cochlear implantation in patients with substantial residual hearing. Laryngoscope. 2004;114:2218–2223. - PubMed
-
- Hodges AV, Schloffman J, Balkany T. Conservation of residual hearing with cochlear implantation. Am J Otol. 1997;18:179–183. - PubMed
-
- von Ilberg C, Kiefer J, Tillein J, et al. Electric-acoustic stimulation of the auditory system. New technology for severe hearing loss. ORL J Otorhinolaryngol Relat Spec. 1999;61:334–340. - PubMed
-
- Gantz BJ, Turner C. Combining acoustic and electrical speech processing: Iowa/Nucleus hybrid implant. Acta Otolaryngol. 2004;124:344–347. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
