

Logistic Organ Dysfunction Score (LODS): a reliable postoperative risk management score also in cardiac surgical patients?
- PMID: 21923900
- PMCID: PMC3184266
- DOI: 10.1186/1749-8090-6-110
Logistic Organ Dysfunction Score (LODS): a reliable postoperative risk management score also in cardiac surgical patients?
Abstract
Background: The original Logistic Organ Dysfunction Sore (LODS) excluded cardiac surgery patients from its target population, and the suitability of this score in cardiac surgery patients has never been tested. We evaluated the accuracy of the LODS and the usefulness of its daily measurement in cardiac surgery patients. The LODS is not a true logistic scoring system, since it does not use β-coefficients.
Methods: This prospective study included all consecutive adult patients who were admitted to the intensive care unit (ICU) after cardiac surgery between January 2007 and December 2008. The LODS was calculated daily from the first until the seventh postoperative day. Performance was assessed with Hosmer-Lemeshow (HL) goodness-of-fit test (calibration) and receiver operating characteristic (ROC) curves (discrimination) from ICU admission day until day 7. The outcome measure was ICU mortality.
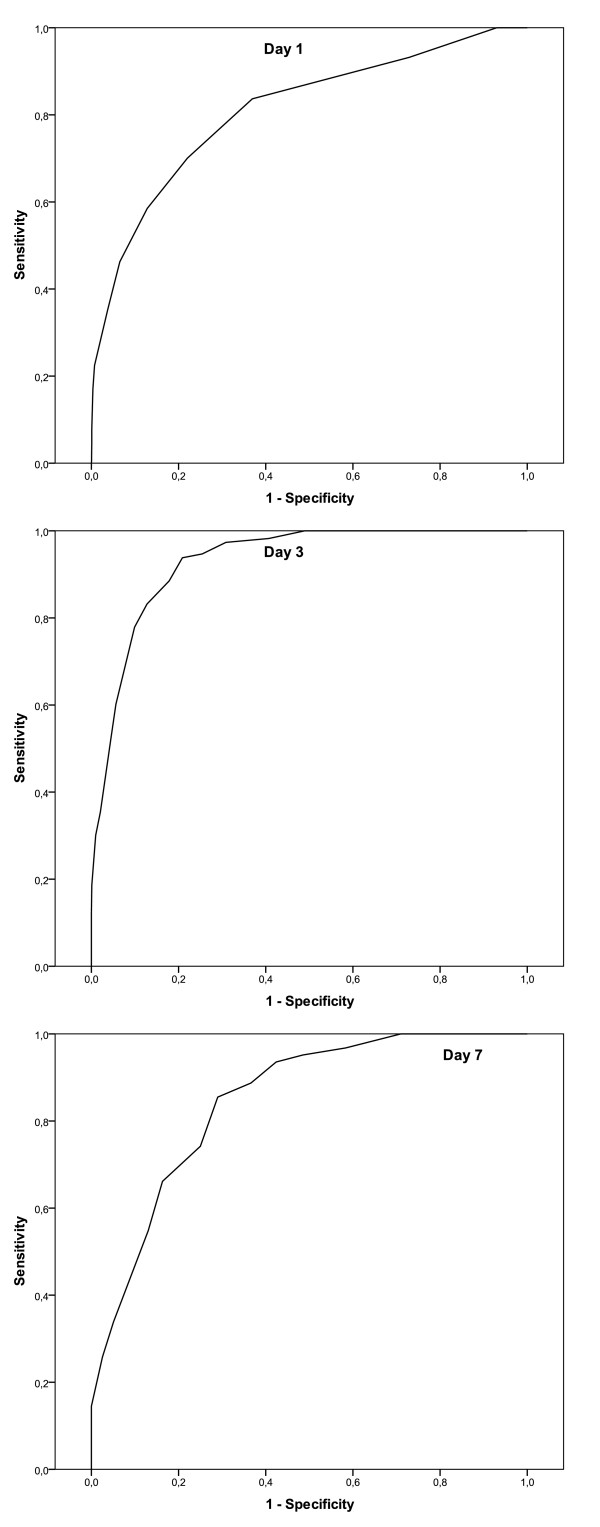
Results: A total of 2801 patients (29.6% female) with a mean age of 66.4 ± 10.7 years were included. The ICU mortality rate was 5.2% (n = 147). The mean stay on the ICU was 4.3 ± 6.8 days. Calibration of the LODS was good with no significant difference between expected and observed mortality rates on any day (p ≥ 0.05). The initial LODS had an area under the ROC curve (AUC) of 0.81. The AUC was best on ICU day 3 with a value of 0.93, and declined to 0.85 on ICU day 7.
Conclusions: Although the LODS has not previously been validated for cardiac surgery patients it showed reasonable accuracy in prediction of ICU mortality in patients after cardiac surgery.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
