

Immunocytology is a strong predictor of bladder cancer presence in patients with painless hematuria: a multicentre study
- PMID: 21924544
- PMCID: PMC3628750
- DOI: 10.1016/j.eururo.2011.08.073
Immunocytology is a strong predictor of bladder cancer presence in patients with painless hematuria: a multicentre study
Abstract
Background: Although the performance of immunocytology has been established in the surveillance of patients with urothelial carcinoma of the bladder (UCB), its value in the initial detection of UCB in patients with painless hematuria remains unclear.
Objective: To determine whether immunocytology improves our ability to predict the likelihood of UCB in patients with painless hematuria. Further, to test the clinical benefit of immunocytology in this setting using decision curve analysis.
Design, setting, and participants: The subjects were 1182 consecutive patients without a history of UCB presenting with painless hematuria and were enrolled at three centres.
Intervention: All patients underwent upper-tract imaging, cystourethroscopy, voided urine cytology, and immunocytology analysis. Bladder tumors were biopsied and histologically confirmed as UCB.
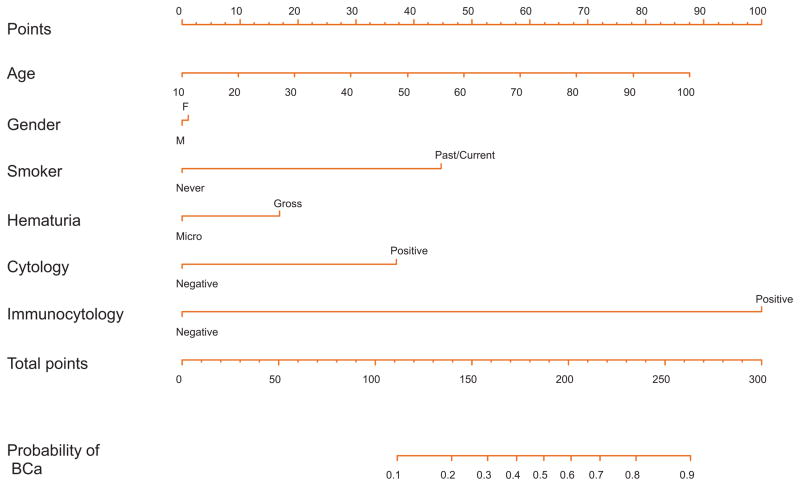
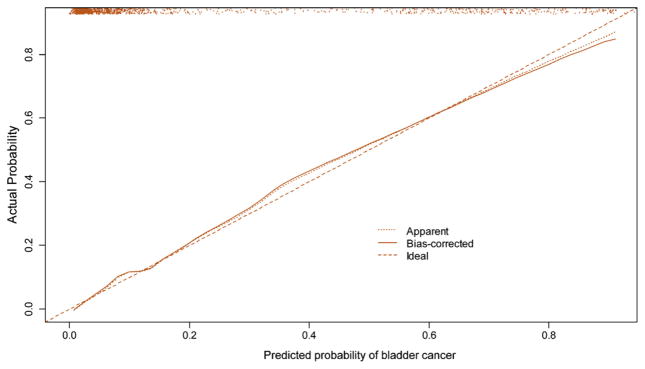
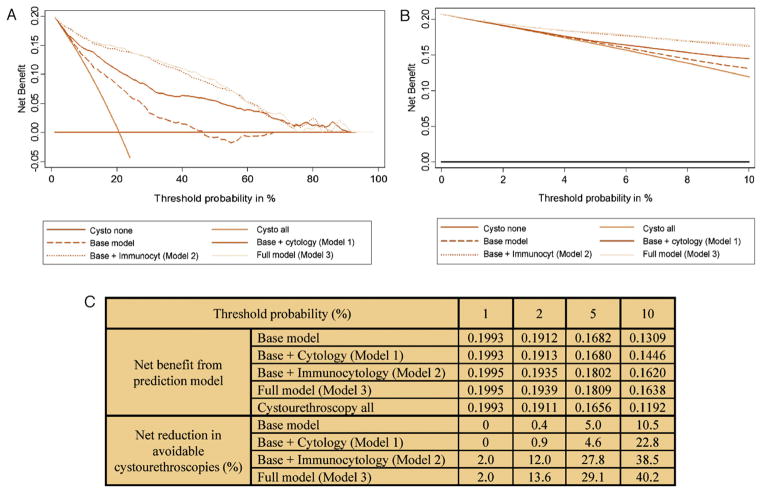
Measurements: Multivariable regression models were developed. Area under the curve was measured and compared using the DeLong test. A nomogram was constructed from the full multivariable model. Decision curve analysis was performed to evaluate the clinical benefit associated with use of the multivariable models including immunocytology.
Results and limitations: Immunocytology had the largest contribution to a multivariable model for the prediction of UCB (odds ratio: 18.3; p<0.0001), which achieved a 90.8% predictive accuracy. Decision curve analysis revealed that models incorporating immunocytology achieved the highest net benefit at all threshold probabilities.
Conclusions: Immunocytology is a strong predictor of the presence of UCB in patients who present with painless hematuria. Incorporation of immunocytology into predictive models improves diagnostic accuracy by a statistically and clinically significant margin. The use of immunocytology in the diagnostic workup of patients with hematuria appears promising and should be further evaluated.
Copyright © 2011 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Grossfeld GD, Litwin MS, Wolf JS, Jr, et al. Evaluation of asymptomatic microscopic hematuria in adults: the American Urological Association best practice policy—part II: patient evaluation, cytology, voided markers, imaging, cystoscopy, nephrology evaluation, and follow-up. Urology. 2001;57:604–10. - PubMed
-
- Babjuk M, Oosterlinck W, Sylvester R, Kaasinen E, Böhle A, Palou-Redorta J. EAU guidelines on non–muscle-invasive urothelial carcinoma of the bladder. Eur Urol. 2008;54:303–14. - PubMed
-
- Johnson EK, Daignault S, Zhang Y, Lee CT. Patterns of hematuria referral to urologists: does a gender disparity exist? Urology. 2008;72:498–502. discussion 502–3. - PubMed
-
- Nieder AM, Lotan Y, Nuss GR, et al. Are patients with hematuria appropriately referred to urology? A multi-institutional questionnaire based survey. Urol Oncol. 2010;28:500–3. - PubMed
-
- Messing EM, Teot L, Korman H, et al. Performance of urine test in patients monitored for recurrence of bladder cancer: a multicenter study in the United States. J Urol. 2005;174:1238–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
