

Glycemic control in non-diabetic critically ill patients
- PMID: 21925080
- PMCID: PMC3718463
- DOI: 10.1016/j.beem.2011.05.004
Glycemic control in non-diabetic critically ill patients
Abstract
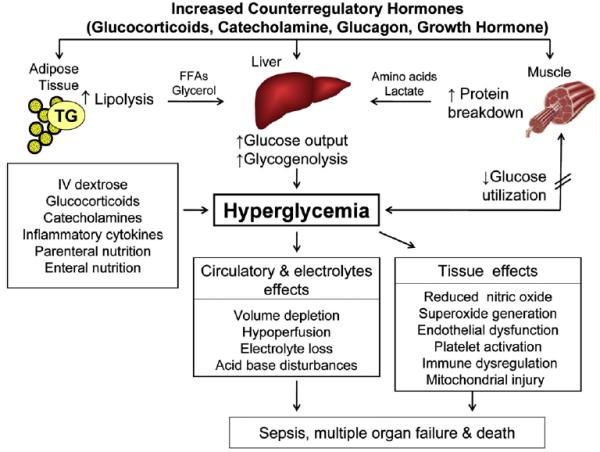
Hyperglycemia is a common and costly health care problem in hospitalized patients. In hospital hyperglycemia is defined as any glucose value >7.8 mmol/l (140 mg/dl). Hyperglycemia is present in 40% of critically ill patients and in up to 80% of patients after cardiac surgery, with ∼ 80% of ICU patients with hyperglycemia having no history of diabetes prior to admission. The risk of hospital complications relates to the severity of hyperglycemia, with a higher risk observed in patients without a history of diabetes compared to those with known diabetes. Improvement in glycemic control reduces hospital complications and mortality; however, the ideal glycemic target has not been determined. A target glucose level between 7.8 and 10.0 mmol/l (140 and 180 mg/dl) is recommended for the majority of ICU patients. This review aims to present updated recommendations for the inpatient management of hyperglycemia in critically ill patients with and without a history of diabetes.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures
References
-
- Organization WH Prevalence of diabetes Worldwide. 2010 vol [World Health Organization website]
-
- Association AD Diabetes Statistics. Diabetes Basics. 2010 vol [American Diabetes Association website]
-
- U.S. Department of Health and Human Services CfDCaP . National estimates and general information on diabetes and prediabetes in the United States. National diabetes fact sheet; 2011.
-
- Xu J, Kochanek KD, Murphy SL, et al. Deaths: Final data for 2007. National vital statistics reports web release. 2010;58(19) - PubMed
-
- Elixhauser AYK, Steiner C, Bierman AS. Hospitalization in the United States, 1997. Agency for Healthcare Research and Quality; Rockville, MD: 2000. HCUP Fact Book No. 1; AHRQ Publication No. 00–0031.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
